Partying with T1D Guide, Part 2
Alcohol and Type 1 Diabetes
Alcohol is the most widely used recreational drug. With type 1 diabetes, it creates a specific failure mode: delayed hypoglycaemia combined with reduced self-rescue. This page explores the mechanism and practical harm-reduction strategies.
Audience. This page is written for adults and older adults living with type 1 diabetes (18+). Alcohol is not a topic GNL covers for infant, preschool, paediatric, or adolescent bands; if you are reading on behalf of a younger person, please refer to your diabetes care team for age-appropriate guidance. Per the GNL age-banding canon, the Alcohol and T1D content refuses every band except adult and older adult.
Before you read
Make sure you have read Part 1: Partying with T1D to understand the shared principles, the inverted U, set and setting, dose uncertainty, and reduced self-rescue.
Listen to Episode 25, Alcohol with T1D with Professor Dessi Zaharieva for the full conversation behind this page.
Download the Alcohol and Type 1 Diabetes FAQ (PDF).
Why alcohol is uniquely risky with T1D
Alcohol is woven into weddings, pubs, festivals, dates, celebrations, and grief. People with type 1 diabetes are part of that world, not outside it.
The risk is usually not one drink. It is a bigger pattern: insulin on board, disrupted sleep, dehydration, late-night eating, and the liver being busy metabolising alcohol instead of supporting glucose stability.
What alcohol does to the brain and body
Alcohol is classified as a depressant (central nervous system slowing), but the early effects can feel stimulating. Two common drivers:
- Dopamine effects that can amplify motivation, reward-seeking, and “keep going” behaviour
- GABA effects that increase inhibition in the brain, driving slurred speech, clumsiness, sedation, and reduced judgement as alcohol accumulates
People react differently. Some become social and energised. Others become emotional, tired, or irritable. That variation is biology, context, and relationship-with-alcohol history. This matters in type 1 diabetes because mood, appetite, and attention directly change glucose decisions.
The liver problem, why alcohol increases hypo risk
The liver prioritises breaking down alcohol, which can reduce its ability to release glucose and defend against falling glucose levels. This is why alcohol is strongly associated with delayed hypoglycaemia, often later in the night and the next morning.
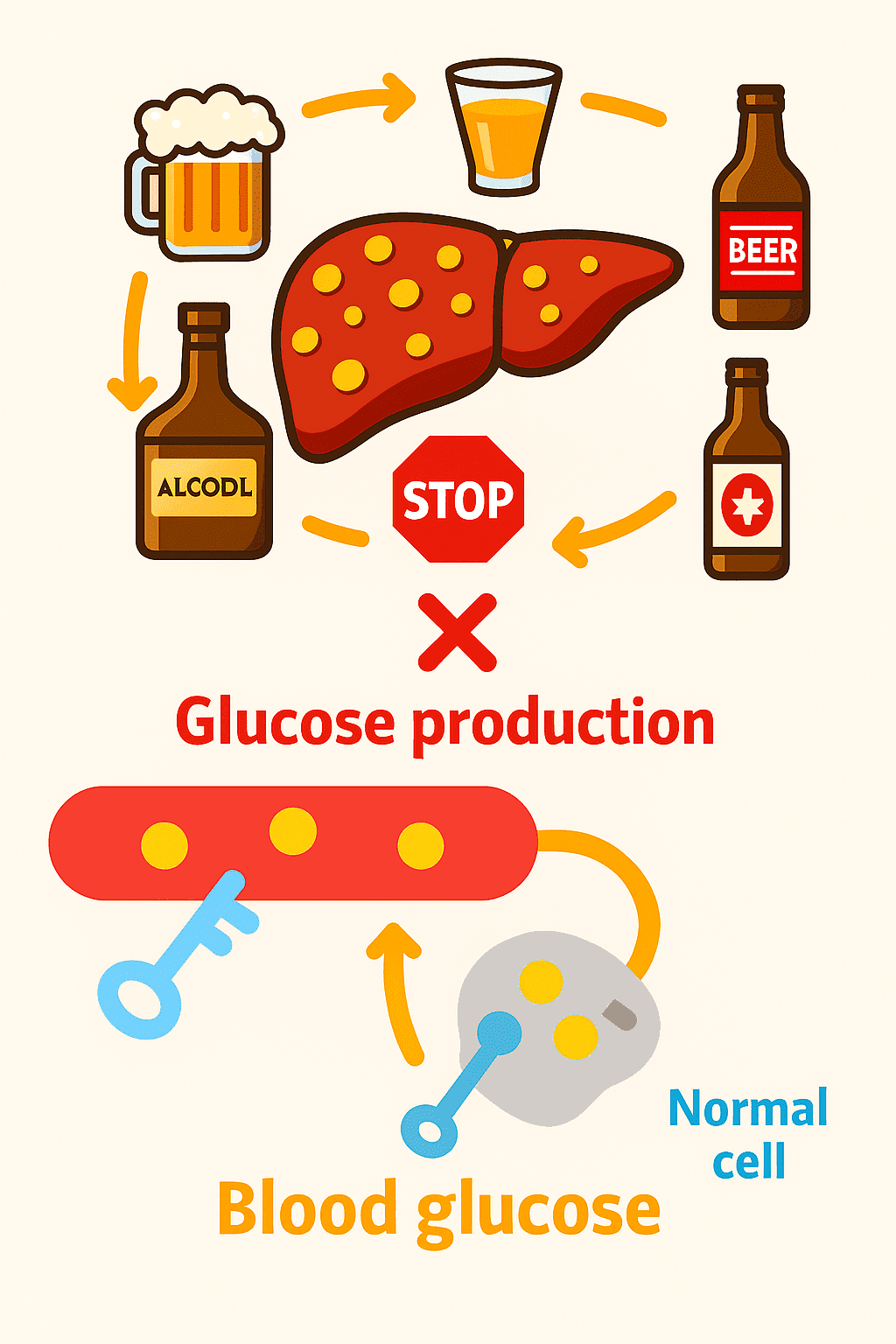
This is a mismatch problem: basal or background insulin keeps working, but the liver’s glucose support may be reduced. That mismatch can drive glucose down when you are least able to notice or treat it.
Glucagon reliability
Glucagon works largely through the liver. If the liver is busy and glycogen stores are limited, glucagon may be less reliable than expected after heavier drinking. This is one reason alcohol nights need an overnight plan, not just a “during the night” plan.
How long does the risk last?
Rules like “one unit equals one hour” are rough heuristics, not physiology. The real answer depends on body size, sex, liver function, food intake, sleep, hydration, activity, and how much insulin is active.
What can be said with higher confidence: delayed hypoglycaemia can occur many hours later, including the next morning, and sometimes well into the next day, especially after heavier drinking.
The core questions to ask before and during
- Roughly how much alcohol am I likely to drink (low, moderate, heavy)?
- Are my drinks mostly no/low carb or carb-containing?
- What therapy am I using (MDI, pump, AID), and how easy is it to reduce insulin safely?
- What is my glucose doing right now (level plus trend), and what insulin is still active?
- What is my overnight plan if I sleep through alarms or symptoms?
Drink categories, carb versus no carb
This is the simplest useful split for glucose management:
- No/low-carb drinks tend to have minimal immediate glucose rise but can carry higher delayed hypo risk later
- Carb-containing drinks can push glucose up initially, then still create a delayed fall later, creating a common trap of over-correcting the initial rise and then going low overnight
No/low-carb drinks
| Drink | Units per drink | Carbs (g) |
|---|---|---|
| Vodka + diet mixer | 1 to 2 | 0 |
| Gin + slimline tonic | 1 to 2 | 0 |
| White wine (dry) | ~2 | ~1 to 2 |
| Red wine | ~2 | ~1 to 2 |
| Tequila / neat spirits | ~1 | 0 |
| White wine spritzer | ~1.5 to 2 | ~2 |
Carb-containing drinks
These can be harder because they create a two-phase problem: early hyperglycaemia risk, later hypoglycaemia risk. If you run an AID system, automatic corrections can stack insulin when you would actually prefer a gentler response overnight.
| Drink | Units per drink | Carbs (g) |
|---|---|---|
| Pint of beer | 2 to 3 | 10 to 15 |
| Cider (dry) | 2 to 3 | 15 to 20 |
| Cider (fruity/sweet) | 2 to 3 | 30 to 40 |
| Alcopops / ready-mix | ~1.5 to 2 | 25 to 40 |
| Sugary cocktails | 1.5 to 2.5 | 20 to 40+ |
| Mixed shots + energy drink | 1 to 2 | 15 to 30 |
Insulin therapy considerations
This section is not a dosing guide. These are the common control levers people discuss with their clinical teams, and typical adjustment ranges reported in lived experience.
On MDI (multiple daily injections)
- Primary lever: the background insulin decision, you cannot turn basal down later the same way as a pump. Typical reductions reported are 25 to 75% on the night of drinking, depending on drinking duration and intensity
- Bolus: for carb-containing drinks and food, many people report using 0 to 50% of their usual bolus dose
- Practical implication: big alcohol nights can be higher risk on MDI because earlier planning is needed
- Clinical discussion: how to safely reduce overnight hypo risk without drifting into sustained hyperglycaemia or ketone risk
On pump therapy
- Primary lever: temporary basal reductions (and when to start them). Typical reductions reported are 25 to 75% before drinking begins, continuing until the morning
- Bolus: for carb-containing drinks and food, many people report using 0 to 50% of their usual bolus dose
- Practical implication: pumps allow faster response to trends, but intoxication can impair judgement and lead to over-adjustment
- Clinical discussion: safe boundaries for temp basal changes and when to avoid correction boluses
On AID / hybrid closed loop systems
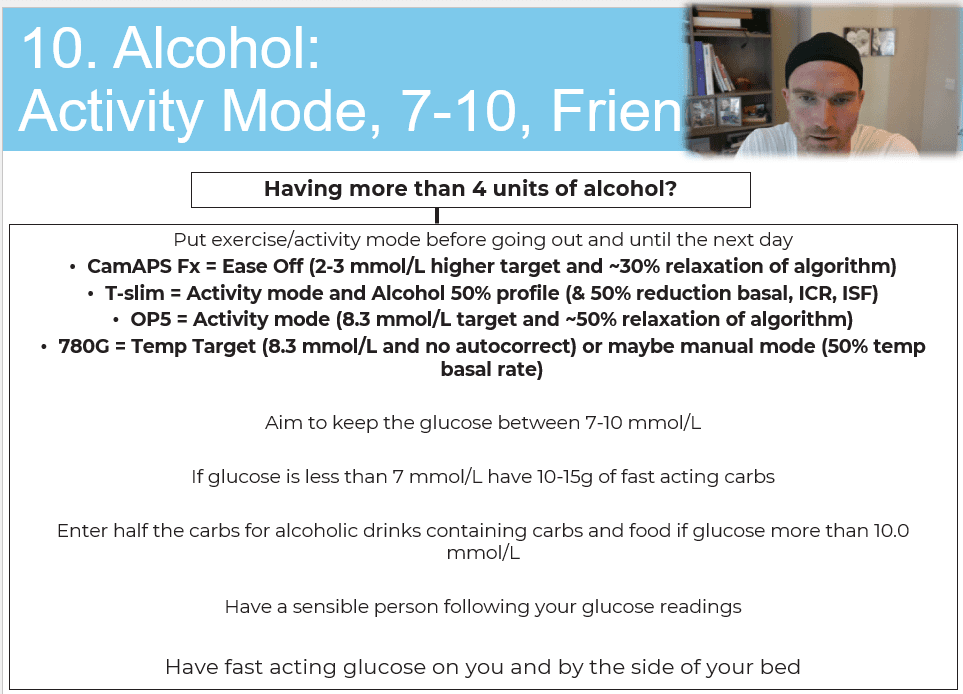
- Primary levers: activity mode or higher targets, and awareness of automated corrections
- Activity mode: turn on before drinking and keep active overnight
- Bolus: for carb-containing drinks and food, many people report using 0 to 50% of their usual bolus dose
- Automatic corrections: carb-heavy drinks or late food can trigger autocorrections that increase delayed hypo risk later
- Manual mode / open loop: may be needed if hypoglycaemia becomes an issue, typically manual mode with 50% usual basal is a starting point people discuss with their team
- Clinical discussion: how to use higher targets safely overnight and when to accept a slightly higher but safe range to reduce severe hypo risk
For AID-specific optimisation: Top tips to optimise time in range with AID systems.
Late-night hunger and the insulin trap
Late-night hunger is common. Alcohol can increase appetite and reduce restraint. This is where many people misjudge insulin: they see a high, eat a lot, or correct aggressively, and then go low later when the liver is still impaired and sleep blunts alarms and symptoms.
Harm-reduction principle from lived experience
When judgement is impaired, bias towards avoiding severe hypoglycaemia. That often means accepting that glucose may run a bit higher overnight, while keeping monitoring and safety tight.
The table below is not a prescription, it illustrates how people tend to think in patterns (glucose band, carb decision, insulin caution):
| Glucose level | Typical carb decision pattern | Insulin caution pattern |
|---|---|---|
| <7 mmol/L (<126 mg/dL) | Eat carbohydrate | Avoid adding insulin when intoxicated |
| 7 to 10 mmol/L (126 to 180) | Small snack or hold | Be cautious with correction |
| >10 mmol/L (>180 mg/dL) | Often avoid extra carbs unless needed | Avoid aggressive corrections |
| If eating more than planned | Consider smaller portions, slower eating | If insulin is used, keep it conservative and clinically discussed |
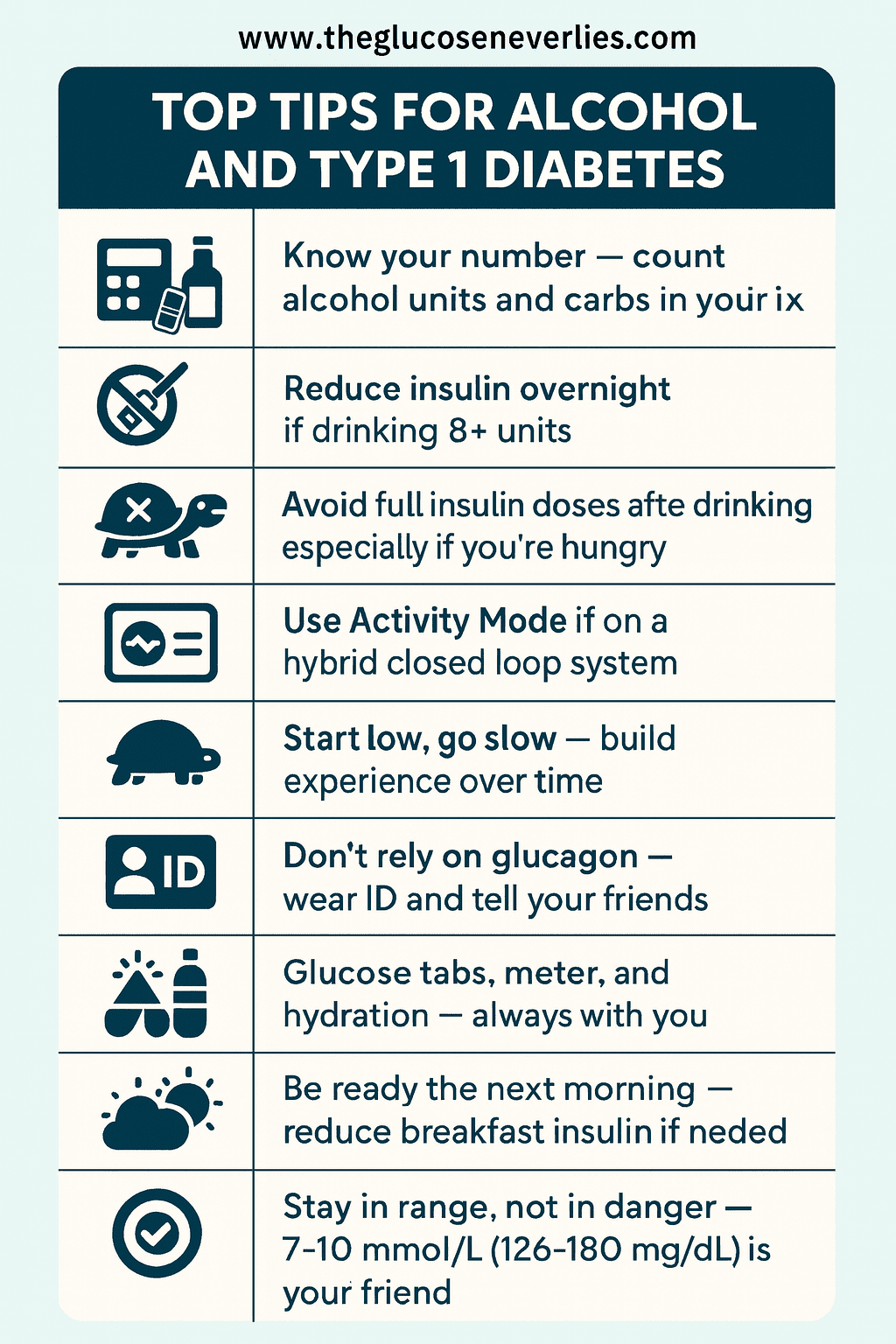
Emergency planning, medical ID, glucagon, and friends
If alcohol is in the mix, plan for the scenario where you cannot self-rescue. That is not pessimism, it is competence.
- Wear medical ID
- Tell at least one person you trust that you have type 1 diabetes and what a severe hypo can look like
- Carry fast-acting glucose
- Consider CGM sharing and location sharing when possible
- Know that glucagon may be less reliable after heavier drinking because the liver may not respond as expected
Festival and big night out kit list
| Item |
|---|
| Glucose tablets |
| Fingerprick meter (CGM alone is not enough) |
| Backup CGM sensor (or two pre-inserted) |
| Medical ID bracelet or card |
| Fast-acting carbs (juice, sweets) |
| Water bottle |
| Insulin pens or syringes (even if on a pump) |
| Portable battery pack |
| Phone with CGM and location sharing on |
| Anti-nausea tablets |
| Spare cannulas |
The minimum viable plan
This is the plan people use when they want to reduce risk without pretending they can control everything:
- Before: eat something; check trend and insulin on board; decide your ceiling for the night (roughly how heavy this might get)
- During: avoid stacking corrections; keep glucose visible; hydrate; tell someone you trust
- Carbs: know whether your drinks are low-carb or carb-heavy; anticipate the two-phase pattern (up then down)
- Overnight: assume you may sleep through symptoms; use CGM sharing and alarms where possible; accept slightly higher targets if needed to avoid severe hypos (especially with AID)
- Morning after: treat it as still in play; monitor longer than you think; delayed hypos are common
Download the Alcohol tips PDF.
What this means in practice
- Alcohol creates a specific mismatch: the liver prioritises alcohol metabolism, reducing its ability to support glucose, while basal insulin keeps working
- Delayed hypoglycaemia is the central risk, often occurring overnight or the next morning
- Drink choice matters: no/low-carb drinks simplify glucose management but still carry delayed hypo risk; carb-containing drinks create a two-phase problem
- Insulin adjustments, whether basal reduction, bolus caution, or AID mode changes, are best discussed with your diabetes care team and tailored to your therapy
- When judgement is impaired, biasing towards avoiding severe hypoglycaemia is worth exploring as the priority
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.