Partying with T1D Guide, Part 3
Stimulants and Type 1 Diabetes
Stimulants increase output, energy, movement, wakefulness, while degrading feedback quality: bodily cues, judgement, appetite, and sleep. That combination can destabilise glucose even when the substance itself does not directly change glucose metabolism.
Before you read
Make sure you have read Part 1: Partying with T1D to understand the shared principles, the inverted U, set and setting, dose uncertainty, and reduced self-rescue.
This page is not a recommendation or endorsement of using any stimulant substance. It does not provide instructions for use. It draws from lived experiences of people with type 1 diabetes, focusing on what tends to happen in the body and in glucose patterns, what can go wrong, and what has reduced harm in practice.
Context from the GNL team: John lived with undiagnosed ADHD until July 2025, which likely shaped his historical pull towards stimulant-driven environments and behaviours. That is not a moral story, it is a reminder that neurobiology and context influence risk, and self-knowledge is part of harm reduction.
The common T1D risk pattern
Across lived experience, the most common risk pattern with stimulants looks like this:
- Movement increases (dancing, walking, pacing), glucose utilisation rises
- Appetite drops or becomes inconsistent, fewer carbs taken in while activity rises
- Adrenaline rises, low symptoms can be masked (“buzzing” does not mean safe)
- Dehydration and overheating, absorption becomes less predictable
- Sleep becomes delayed or lost, next-day insulin resistance, mood vulnerability, care fatigue
- Alcohol often co-occurs, delayed hypoglycaemia risk becomes the highest-stakes window overnight
Everything on this page points back to two concepts: the inverted U (each stimulant has a narrow manageable zone and a steep drop-off) and dose uncertainty (with unregulated substances, numbers can create false confidence).
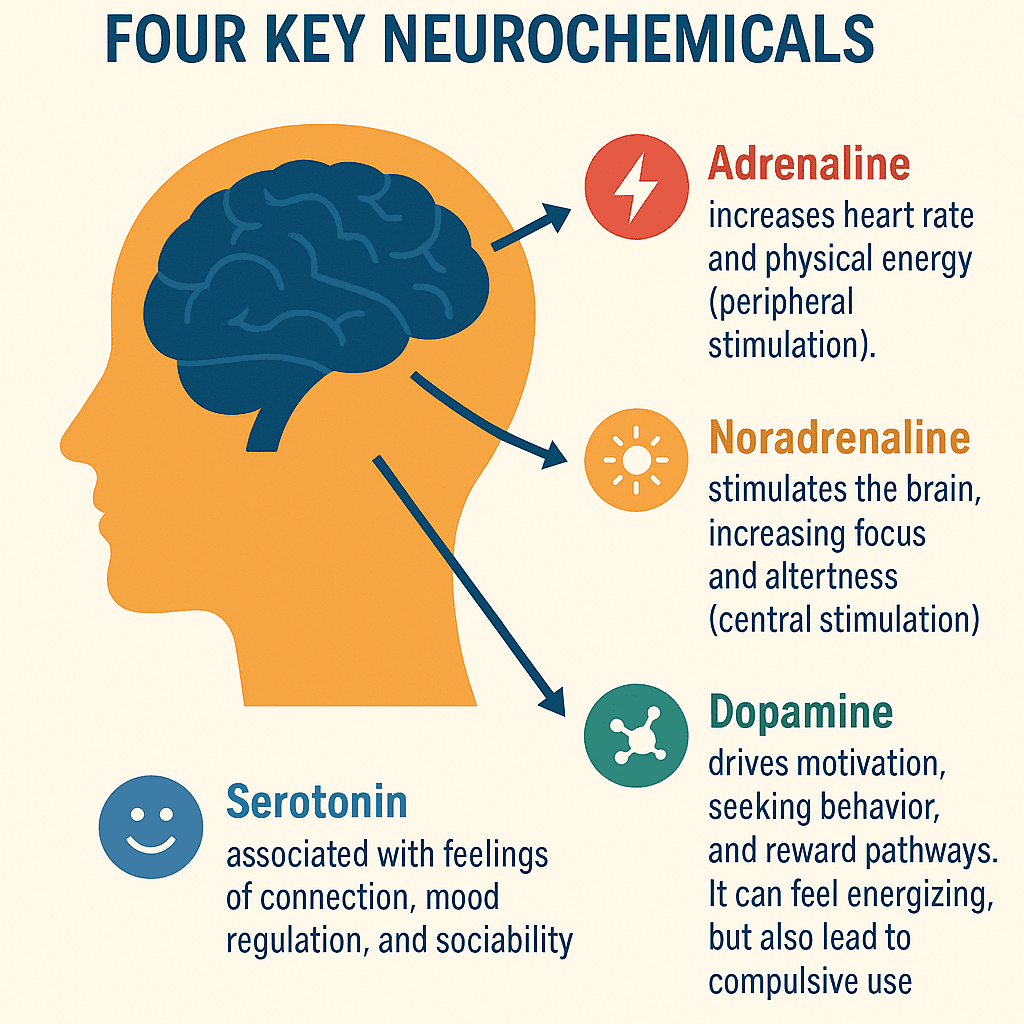
Shared neurochemistry
Most stimulants work by altering the signalling of a few key systems, especially dopamine (drive and reward), noradrenaline and adrenaline (arousal and activation), and for some substances, serotonin (connection and mood). This is why people often report energy, confidence, talkativeness, reduced fatigue, and reduced appetite.
The problem is not just the neurochemistry. It is the behavioural cascade that follows: more movement, less eating, less sleep, more risk-taking, and less reliable self-monitoring.
The inverted U, why dose matters
Stimulants operate on an inverted U-curve: too little does nothing, a middle range produces the effect people seek, and beyond that peak the same substance can produce anxiety, agitation, panic, paranoia, overheating, and unsafe decisions. The curve shifts depending on sleep, hydration, mood, food, tolerance, and mixing substances.
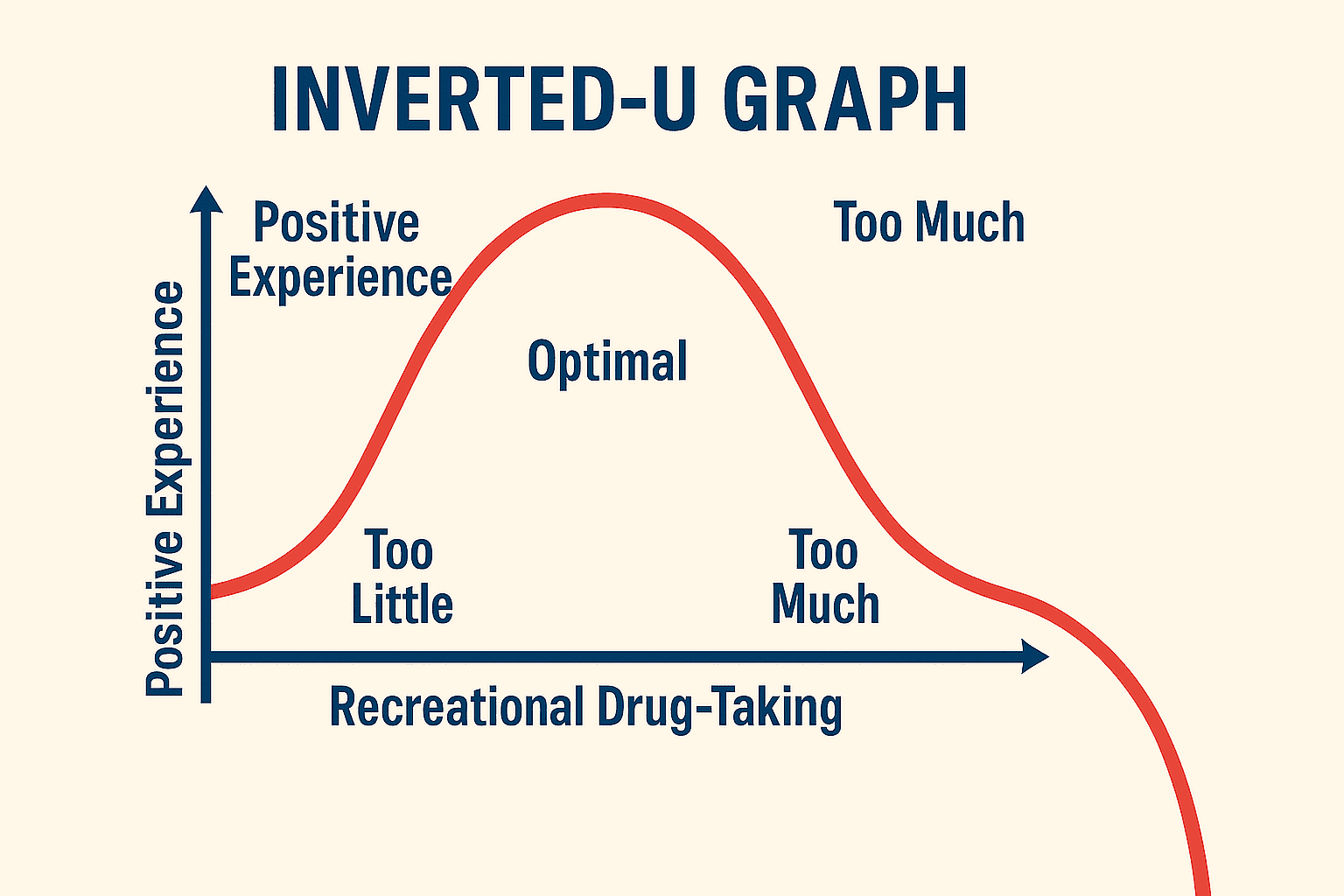
For unregulated substances, numbers do not protect you because potency and adulterants may be unknown. Any dose information below is provided only to make the inverted U concept concrete, not to guide use.
Regulated stimulants, caffeine and nicotine
Caffeine and nicotine are regulated and labelled, which makes the inverted U easier to manage. The risk is still real when combined with sleep deprivation, dehydration, anxiety, or alcohol.
Caffeine and T1D
Caffeine is the most widely used stimulant in the world. In party settings, it is often used to stay alert or counteract alcohol’s sedating effects. Mechanistically, caffeine increases alertness by blocking adenosine signalling (a key fatigue signal) and can increase adrenergic tone.
In type 1 diabetes, caffeine rarely causes a predictable glucose effect on its own. The bigger issue is what it enables: more movement, later nights, less sleep, and less structured eating, all of which can increase variability and late-night risk.
| Product | Caffeine content |
|---|---|
| 1 cup of coffee (240 mL) | 80 to 100 mg |
| Red Bull (250 mL) | 80 mg |
| Monster Energy (500 mL) | 160 mg |
| ProPlus tablet | 100 mg |
| Double espresso | 120 to 150 mg |
| Pre-workout shot (1 serving) | 200 to 300+ mg |
| Diet Coke (330 mL) | 40 mg |
Nicotine and T1D
Nicotine is a regulated stimulant found in cigarettes, vapes, patches, gum, lozenges, and pouches. Nicotine’s biggest risk is not acute glucose disruption, it is addictive potential and the way adrenergic stimulation can mask bodily cues, including hypoglycaemia symptoms. Tolerance builds quickly with repeated use.
| Product type | Typical nicotine content |
|---|---|
| Cigarette (1) | ~1 to 2 mg absorbed |
| Nicotine gum (1) | 2 to 4 mg |
| Nicotine lozenge (1) | 2 to 4 mg |
| Nicotine pouch | 4 to 10 mg |
| Nicotine patch (per 24 hours) | 7 to 21 mg |
Vaping exposures vary widely with device and puffing pattern, so milligrams absorbed are hard to estimate from a label alone.
Unregulated stimulants, the common failure modes
This section covers cocaine, MDMA, and amphetamines at the level of physiology and T1D-relevant risk patterns. The highest-risk patterns are predictable system failures:
- Alcohol co-use, delayed hypoglycaemia risk rises substantially overnight
- Continuous movement, glucose utilisation increases while appetite and attention decrease
- Adrenaline masking lows, “buzzing” can hide a falling glucose
- Overheating and dehydration, higher stress and more variable insulin absorption
- Sleep loss, next-day insulin resistance, mood vulnerability, care fatigue
- Compulsive loops (especially with short-acting stimulants), escalating beyond the manageable zone
Dose bands, making the inverted U concrete
The table below is illustrative, not prescriptive. It exists to explain why overshooting happens and why “a bit more” can flip the experience from energised to unsafe. With unregulated substances, the same milligram number can sit anywhere on the U-curve depending on purity, adulterants, tolerance, sleep, hydration, and mixing.
| Substance | Lower exposure band | Moderate exposure band | Higher exposure band |
|---|---|---|---|
| MDMA (total over an event) | ~40 to 75 mg | ~75 to 125 mg | >125 to 200+ mg |
| Amphetamine-type stimulants (total over an event) | ~5 to 15 mg (pharma-equivalent) | ~15 to 30 mg | >30 mg+ |
| Cocaine (highly variable) | Lower exposure | Moderate exposure | High exposure |
Cocaine exposure estimation is unreliable because the product is often adulterated and delivered in inconsistent amounts. The more useful framing is not milligrams, it is the behavioural loop (short-lived effects, repeated re-dosing, overshooting the curve).
Substance-specific patterns
MDMA and T1D, movement, heat, dehydration, and the crash
MDMA is commonly reported to increase emotional openness, sensory intensity, and movement. In type 1 diabetes, risk is usually driven by behaviour: long periods of dancing, reduced appetite, dehydration and overheating, and delayed sleep.
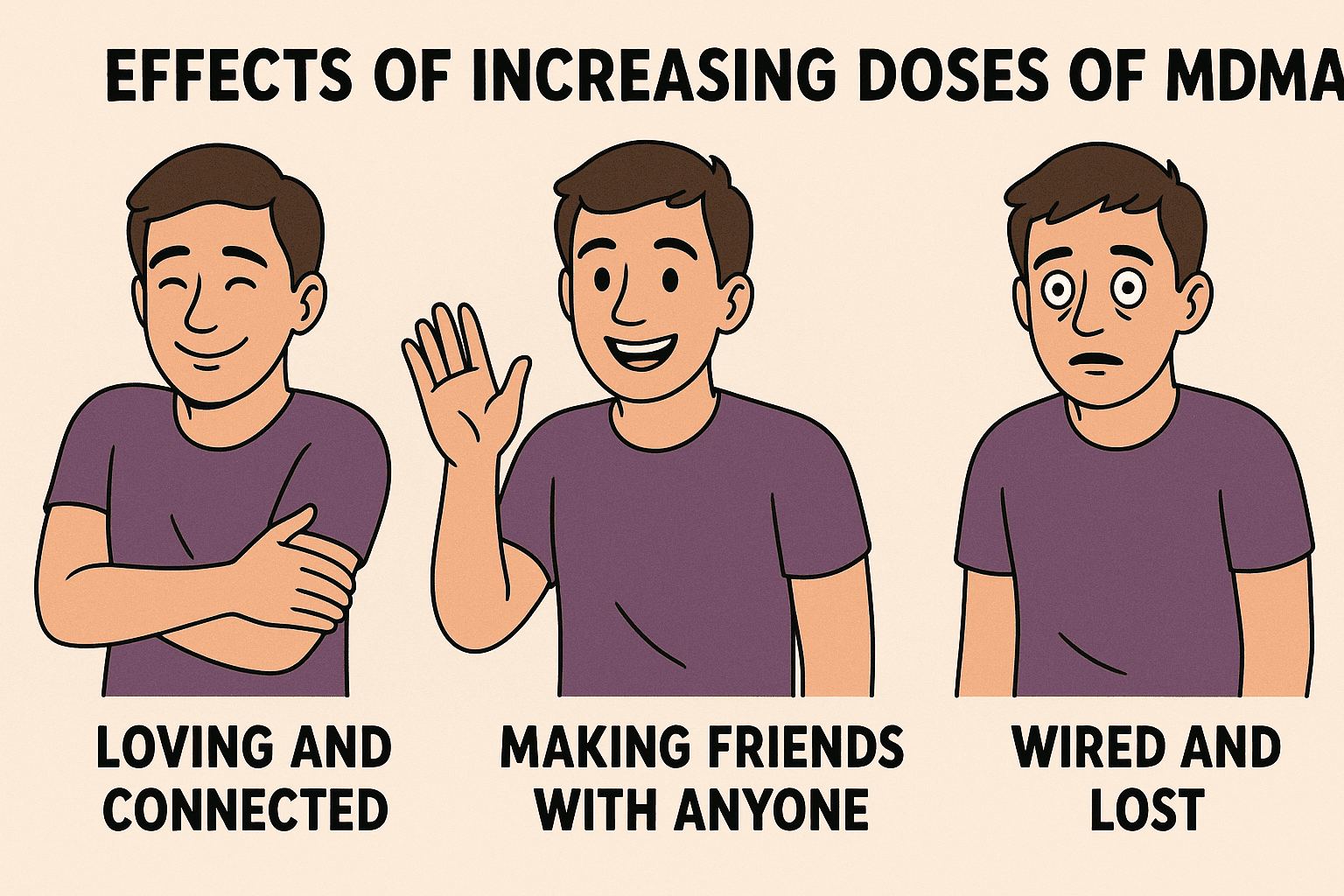
A commonly reported after-effect is a low mood and flatness period in the days afterwards. In type 1 diabetes, this matters because low mood plus poor sleep plus disrupted routine increases the chance of missed meals, missed boluses, poor monitoring, and reduced self-care bandwidth.
Amphetamines and T1D, long duration, low sleep, high variability
Amphetamines are often described as long-lasting stimulation: prolonged wakefulness, reduced fatigue signals, reduced appetite, and sustained drive to move and talk. In type 1 diabetes, the key risk is duration, the longer you stay awake and active, the longer you have to manage glucose while decision quality degrades.
Sleep loss is a core driver of next-day glucose volatility. Many people report higher insulin resistance, poorer appetite regulation, and emotional fragility after stimulant nights, even when nothing bad happened acutely.
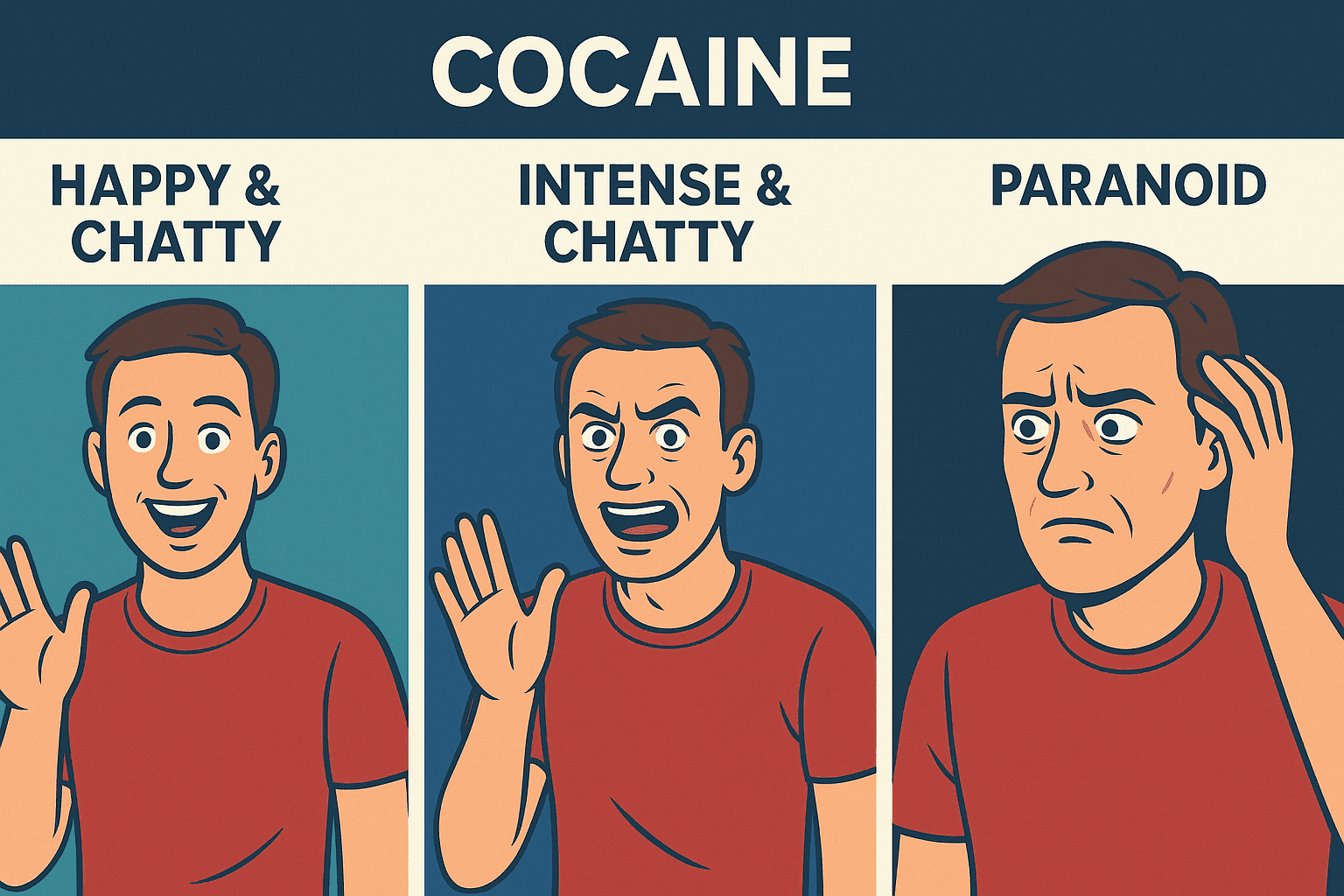
Cocaine and T1D, short-acting loops and alcohol stacking
Cocaine is often described as intense and short-acting, which can create a loop of repeated re-dosing. In lived experience, the biggest type 1 diabetes risks are environmental: increased alcohol intake, reduced awareness of lows, prolonged wakefulness, and next-day crash states that undermine self-care.
A critical high-risk pattern is stimulant plus alcohol: stimulants can mask alcohol sedation, leading to more drinking, which then increases delayed hypo risk overnight.
Risk summary
| Risk area | T1D-specific concern |
|---|---|
| Movement increases | Higher glucose utilisation and increased hypo risk |
| Adrenaline masking | Lows can feel like “buzzing” or anxiety |
| Reduced eating | Less carb intake while activity increases |
| Overheating and dehydration | Higher physiological stress and variable insulin absorption |
| Sleep loss | Next-day insulin resistance, mood vulnerability, care fatigue |
| Alcohol stacking | Higher delayed hypo risk overnight |
| Post-event crash | Lower self-care capacity for 1 to 4 days |
Minimum viable harm-reduction plan
This will not make stimulant use safe, but it can reduce predictable failure modes in type 1 diabetes:
- Do not go in depleted: eat beforehand, hydrate, and start with a stable glucose trend
- Keep glucose visible: use CGM alerts where possible and consider sharing CGM data with someone you trust
- Assume you will move more than you think: dancing and walking are the common hidden drivers of unexpected lows
- Carry hypo treatment: fast carbs you can take even when you do not feel like eating
- Tell at least one person: someone should know you have type 1 diabetes and what severe hypoglycaemia can look like
- Plan for sleep loss: expect next-day insulin needs and mood to shift, build recovery time
- Alcohol multiplies risk: if alcohol is involved, treat overnight delayed hypoglycaemia as the main threat window
Download the Taking stimulants with T1D safety guide (PDF).
What this means in practice
- Stimulants increase output while degrading the feedback loops that keep glucose management stable, movement, appetite, sleep, and self-monitoring all change
- The inverted U applies to all stimulants: a narrow manageable zone and a steep drop-off into anxiety, overheating, or unsafe decisions
- With unregulated substances, dose uncertainty means milligram numbers can create false confidence
- The biggest real-world risk pattern is often substance plus alcohol plus sleep loss, not any single drug in isolation
- Planning for the behavioural cascade (not just the pharmacology) is what tends to reduce harm most reliably
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.