Exercise and Type 1 Diabetes
Making exercise predictable enough to manage, without pretending it can ever be perfectly controlled. From ten minutes after a meal to training for an endurance event: the same physiology, the same three variables.
TL;DR
- Insulin on board is the dominant driver of exercise hypo risk; the 90-minute window and Three-Hour Rule are how you manage it.
- Activity and exercise are not the same thing. Ten to twenty minutes of everyday movement after meals is a distinct, lower-risk lever for smoothing glucose that most people underuse.
- Three variables decide almost everything: insulin on board, starting glucose, trend arrows. Address these first before adjusting anything else.
- AID changes the levers but not the physics. Announcing exercise and pre-emptive reductions matter more, not less, on an AID system.
- Read Part 3 if you want to understand how twenty minutes of moderate post-meal activity can blunt a postprandial rise without triggering a later hypo.
Work through the eight sections below. They climb from Foundations (with Jude), through Advanced (with Grace), into Mastery (with John). Progress is stored only in your own browser (localStorage), no account, no server, no data leaves this page.
1What exercise is, and why it destabilises T1DThe beginner on-ramp: fast physiology meeting slow insulin, and the activity-versus-exercise distinction
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The guide says exercise in type 1 diabetes is often called 'unpredictable', then argues that conclusion is usually wrong. What is its alternative explanation for why glucose moves so sharply during exercise?
2The page draws a distinction between 'activity' and 'exercise'. What is the distinction, and why does it change how each is managed?
3The guide names the variables that predict an exercise low, in order, with exercise type coming last. What is that order, and why does exercise type come after the others?
What this guide is for
Exercise is not random. It is fast physiology meeting slow insulin.
For people living with type 1 diabetes, exercise can feel uniquely destabilising: drops that arrive fast and hard, spikes that linger, sessions that look identical on paper but behave very differently in real life. The common conclusion is that exercise is “unpredictable”. That conclusion is understandable, and usually wrong.
Exercise does not introduce randomness. It introduces fast, powerful physiology into a system otherwise governed by slow, blunt insulin. When you understand the dominant drivers, patterns appear; and with them, a clearer picture.
This guide is built around heuristics to experiment from. Grounded in the evidence base (EASD/ISPAD 2025 consensus, ISPAD exercise chapter, GNL’s own causal modelling), tailored by individual response. They are not rigid rules. They are starting points that survive contact with CGM and real life.
Activity versus exercise
Not all movement requires a full plan
Exercise and everyday activity are not the same thing, and the distinction matters for how you manage glucose.
Activity is everyday movement: walking, light cycling, housework, gardening, playing with children. It is not training. The point is not fitness. The point is glucose leverage. Activity works best as an add-on to normal life; you do not need to be an exercise person to use it.
The contrast matters because the management demands are different:
- Activity: lower hypoglycaemia risk, easier to repeat, well suited to glucose smoothing and post-meal peaks.
- Exercise: higher potential benefit for fitness and performance, but typically requires more deliberate glucose management before, during, and after.
Starting with activity snacking (ten to twenty minutes after the meal that produces your biggest spike) is often the most accessible entry point, particularly for families and children who find formal exercise management daunting.
Major in the majors
Four variables decide almost everything
If exercise has felt chaotic, start here. Across almost all forms of exercise, what predicts an exercise low comes down to a short list, in order. Exercise type matters, but it is fourth; the three starting conditions come first.
1 · Strongest predictor
Glucose value
Where you start shapes where you land. The pre-exercise glucose is the single strongest predictor of a low.
2
Trend arrow
Direction and speed of change. A number without a trend is incomplete.
3
Insulin on board
Recent bolus insulin is the dominant lever you control; the 90-minute window and Three-Hour Rule are how you manage it.
4
Exercise type
Aerobic tends to lower glucose, anaerobic can raise it. It shapes the plan, but comes after the three starting conditions.
When these are checked in order, exercise stops being mysterious and starts becoming manageable. Most exercise-related hypoglycaemia and volatility is predictable from these starting conditions (Bergford 2023).
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The guide says exercise in type 1 diabetes is often called 'unpredictable', then argues that conclusion is usually wrong. What is its alternative explanation for why glucose moves so sharply during exercise?
Reveal answer
Exercise does not introduce randomness; it introduces fast, powerful physiology into a system otherwise governed by slow, blunt insulin. Working muscle pulls glucose out of the blood quickly, blood flow speeds up absorption of insulin that is already injected or pumped, and the result is that the insulin already present is amplified. Injected insulin cannot respond at the same speed, so the apparent chaos is fast physiology meeting slow insulin, not luck. When the dominant drivers are understood, patterns appear. This is a concept to understand, not an instruction to act on.
2The page draws a distinction between 'activity' and 'exercise'. What is the distinction, and why does it change how each is managed?
Reveal answer
Activity is everyday movement (walking, light cycling, housework, gardening, playing with children); its point is glucose leverage rather than fitness, and it carries lower hypoglycaemia risk, so it is easier to repeat and well suited to smoothing post-meal peaks. Exercise is structured training with higher potential fitness benefit but typically needs more deliberate glucose management before, during and after, because the hypoglycaemia risk is higher. The skill is matching the tool to the situation rather than applying a full exercise protocol to every short walk. Understanding the distinction is the learning point.
3The guide names the variables that predict an exercise low, in order, with exercise type coming last. What is that order, and why does exercise type come after the others?
Reveal answer
In order of how strongly each predicts an exercise low: the glucose value first (the pre-exercise glucose is the single strongest predictor), then the trend arrow (direction and speed of change), then insulin on board (the dominant lever you control), with exercise type fourth. This is the Bergford 2023 ordering. The reason exercise type comes after the three starting conditions is that across almost all forms of exercise these conditions dominate whether glucose falls, so most exercise-related hypoglycaemia is predictable from them; exercise type then tells you which direction to plan for. The framing is ‘major in the majors’: check the first three before adjusting anything else. It is a way of organising attention, not a personalised plan, and any change to insulin is a care-team decision.
2Your first plan: safety basics and carbsThe beginner plan that changes no insulin: the hypo and insulin-on-board basics, fast-acting carbs ready, and roughly how many a 30-minute session needs (from the explorer)
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1Before any session, the plan covers two safety basics: what a hypo is and what insulin on board is. Why does insulin on board matter so much for exercise, and when can an exercise low show up?
2Before changing any insulin, what is the simplest first plan for exercising safely, and why is carbohydrate a sensible lever to start with?
3The carb cards show that a thirty-minute gentle session needs more carbohydrate as body weight rises. Why is the amount tied to weight, and why is it a starting point rather than a fixed dose?
Before you start: the safety basics
Two things to have clear before any session. First, a hypo is a low glucose. Exercise makes lows more likely, and they can arrive late: during the session, in the one to two hours afterwards, and overnight after evening exercise. That is why the plan starts with having fast-acting carbohydrate ready, and why a severe low always needs help from someone else. The shape to remember is recognise it, treat it with fast carbs, then recheck. How much fast carb is itself weight-scaled rather than a fixed number, which is the same logic the carb cards below use; the hypoglycaemia guide covers the weight-based amount in full.
Second, your insulin on board. This is the still-active part of a recent mealtime dose (a bolus), and it is the single biggest reason glucose falls during exercise, because activity makes that insulin work harder. So the timing of a session relative to your last bolus matters, which is why insulin on board is one of the three things to check before you move.
These are general ideas to understand, not personalised instructions; your own plan is made with your care team.
Your first plan: carbohydrate for a session
You do not need to change any insulin to start exercising safely. The simplest, safest first plan is to have fast-acting carbohydrate ready and to know roughly how much a session might need, so a fall does not catch you out. Carbohydrate is the beginner’s lever: it works fast, it is forgiving, and it asks nothing of your pump or pen settings.
The cards below come straight from the GNL Exercise IOB explorer: roughly how many carbs a thirty-minute gentle (aerobic) session needs when there is only a light amount of insulin on board (about 0.05 units per kg), across body weights. They are population-average starting points to understand, not personal doses; you learn your own pattern with CGM and your care team.
- 3 g glucose tablets: 2 tablets
- 4 g glucose tablets: 1 tablet
- Grapes: about 3 grapes
- Fruit juice: about 100 mL
- 3 g glucose tablets: 4 tablets
- 4 g glucose tablets: 3 tablets
- Grapes: about 7 grapes
- Fruit juice: about 100 mL
- 3 g glucose tablets: 5 tablets
- 4 g glucose tablets: 4 tablets
- Grapes: about 11 grapes
- Fruit juice: about 200 mL
- 3 g glucose tablets: 7 tablets
- 4 g glucose tablets: 6 tablets
- Grapes: about 15 grapes
- Fruit juice: about 200 mL
- 3 g glucose tablets: 9 tablets
- 4 g glucose tablets: 7 tablets
- Grapes: about 17 grapes
- Fruit juice: about 300 mL
The Carbs for 30 Minutes Exercise explorer lets you put in your own weight, glucose, trend and recent insulin and see the estimate for your situation. Start here; the insulin-reduction levers come later, once the carb plan feels familiar.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1Before any session, the plan covers two safety basics: what a hypo is and what insulin on board is. Why does insulin on board matter so much for exercise, and when can an exercise low show up?
Reveal answer
Insulin on board is the still-active part of a recent mealtime dose, and it is the biggest single reason glucose falls during exercise, because activity makes that insulin work harder; that is why the timing of a session relative to your last bolus matters. An exercise low is not only a during-exercise risk: it can arrive late, in the one to two hours after a session and overnight after evening exercise, which is why having fast carbohydrate ready and rechecking afterwards are part of the basic plan. These are general ideas to understand, not personalised instructions, and the personal plan is made with the care team.
2Before changing any insulin, what is the simplest first plan for exercising safely, and why is carbohydrate a sensible lever to start with?
Reveal answer
The simplest first plan is to have fast-acting carbohydrate ready and to know roughly how much a session might need, so a fall does not catch you out. Carbohydrate is a good lever to start with because it works quickly, it is forgiving, and it asks nothing of your pump or pen settings: you do not have to change any insulin to begin exercising safely. The insulin-reduction levers come later, once the carbohydrate plan feels familiar. This is a general starting plan to understand, not a personalised dose, and the amount is explored with CGM and the care team.
3The carb cards show that a thirty-minute gentle session needs more carbohydrate as body weight rises. Why is the amount tied to weight, and why is it a starting point rather than a fixed dose?
Reveal answer
More body weight generally means more working muscle pulling glucose out of the blood during exercise, so a larger person tends to need more fuel for the same session; the cards reflect that by scaling the carbohydrate with weight at a light insulin load. It is a starting point rather than a fixed dose because the real amount also depends on insulin on board, the type and intensity of exercise, the time of day and individual variation, so the population-average figure is a place to begin and then refine with CGM data and the care team, who own any change to the plan.
3How exercise moves glucose (the mechanism)Insulin amplification, myokines, and why exercise type explains direction
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The guide says contracting muscle takes up glucose through a pathway that does not need insulin. What is that mechanism, and why does it mean exercise lowers glucose even when very little insulin is around?
2Why does the guide say people with type 1 diabetes are disproportionately vulnerable to exercise-induced hypoglycaemia, compared with people without diabetes?
3The guide says different exercise types tend to push glucose in different directions. What is the broad pattern for aerobic versus anaerobic exercise, and what mechanism drives the difference?
Part 1 · Anchor thesis
Exercise amplifies insulin action. That is the whole story.
Muscle contraction pulls glucose out of the blood through pathways that are largely insulin-independent. Blood flow rises, insulin already injected or pumped is absorbed faster, and glucose uptake accelerates. The apparent chaos of exercise in type 1 diabetes is not randomness; it is fast physiology meeting slow insulin.
Once you know how the mechanism works, the rest of the guide becomes a set of levers rather than a list of rules. Everything in Parts 2, 3 and 4 traces back to this Part.
Major in the majors
Three variables decide almost everything
Across almost all forms of exercise, glucose behaviour is dominated by three variables, in order of importance. This is the control order, the lever you move first; it is the same short list as the predict-a-low order in Part 1, just ranked for acting rather than forecasting, so insulin on board leads here.
1 · Most important
Insulin on board
Recent bolus insulin is the dominant driver of exercise hypo risk.
2
Starting glucose
Where you start shapes where you land, especially for aerobic work.
3
Trend arrows
Direction and speed of change. Numbers without direction are incomplete.
The mechanism in plain terms
Working muscle needs fuel. Contracting muscle fibres translocate GLUT4 glucose transporters to the cell surface through calcium- and contraction-driven pathways that do not require insulin. Sylow and colleagues describe this as the dominant pathway of exercise glucose uptake; which is why exercise lowers glucose even in near insulin-deficient states.
At the same time, blood flow to working muscle and skin increases several-fold. Any injected or pumped insulin already in subcutaneous tissue is absorbed faster. The net result is that circulating insulin rises at the moment muscle is most sensitive to it. Exercise does not inject extra insulin; it supercharges the insulin that is already there.
Counter-regulation is real but blunted in T1D
In people without diabetes, liver glucagon release and sympathetic drive push glucose out of storage to match muscle demand. In type 1 diabetes, the alpha-cell glucagon response is blunted (Colberg 2022). This is one of the primary reasons people with T1D are disproportionately vulnerable to exercise-induced hypoglycaemia; counter-regulation is not doing its usual job.
Myokines: muscle as an endocrine organ
Severinsen and Pedersen (2020) review myokines, the proteins released by contracting muscle that act on other tissues. Regular exercise is not only about the glucose curve on the day. It is about the slower, cumulative benefits that follow repeated contraction. This is the non-glycaemic case for activity.
Exercise type explains direction
Different modalities tend to move glucose in different directions. The three majors still decide risk; but exercise type tells you what risk to plan for.
| Type | Typical glucose response | Mechanism |
|---|---|---|
| Aerobic (running, cycling, swimming) | Tends to lower | Sustained muscle glucose uptake dominates |
| Anaerobic (sprinting, heavy lifting) | Often rises | Catecholamine and cortisol release push glucose out of the liver |
| Mixed / team sports | Can rise or fall | Depends on intensity balance and IOB at the start |
The 10-second sprint trick
Bussau et al (2006) showed that a single maximal sprint at the end of moderate exercise triggers enough catecholamine response to blunt the post-exercise glucose decline. This is mechanism translated directly into a practical tool. When aerobic exercise is dropping glucose faster than wanted, a short, very hard effort can lift glucose without requiring carbohydrate.
Iscoe and Riddell showed the same principle holds for brief high-intensity intervals dropped inside continuous moderate exercise.
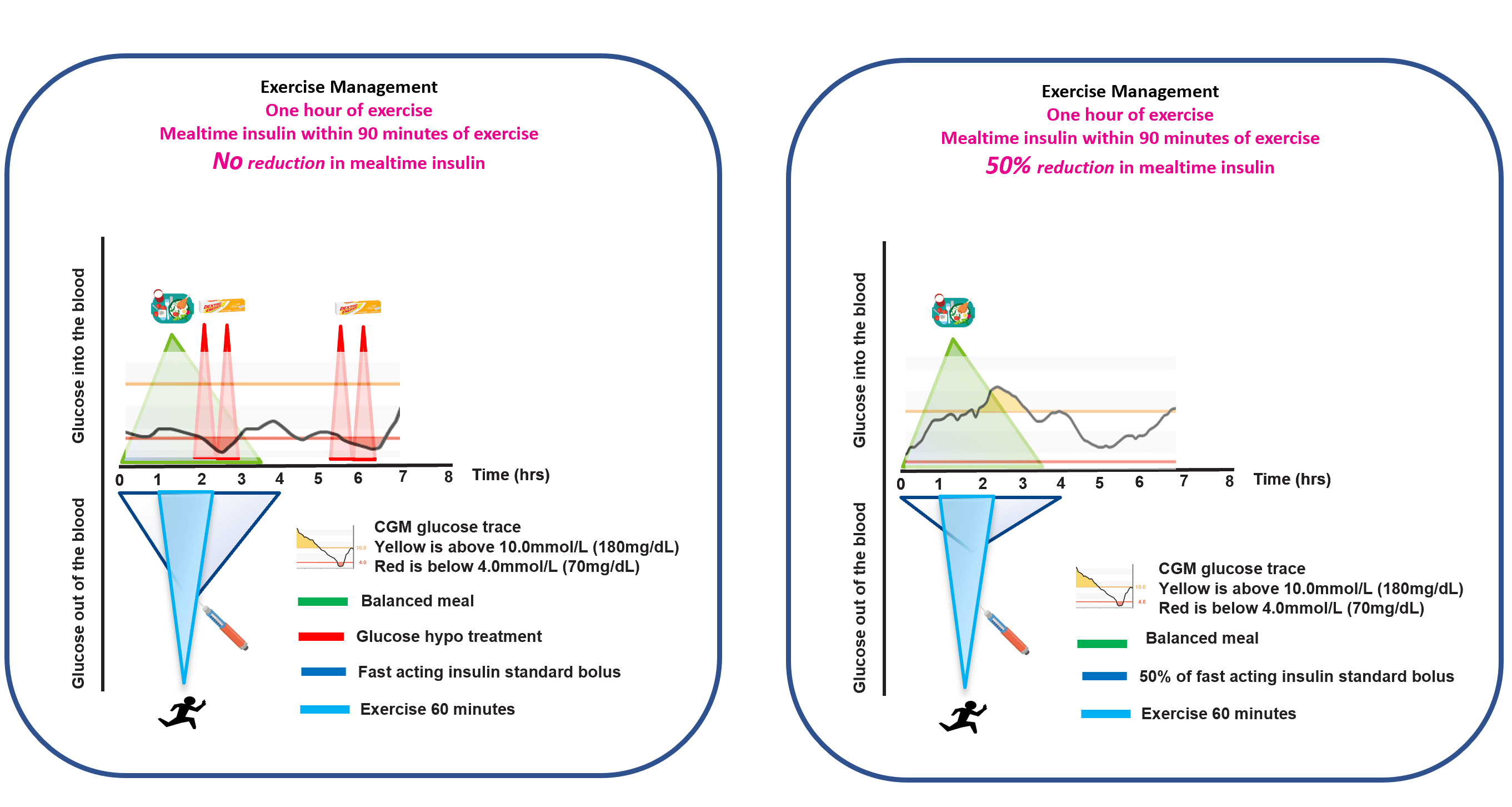
The 90-minute window
When exercise begins within roughly ninety minutes of a meal bolus, insulin action is often near its peak. In this window, rapid-acting analogues are doing their heaviest work and exercise is amplifying every unit of it. This is where the largest, fastest drops tend to happen.
A common starting point is that exercise planned within the 90-minute window after a meal bolus usually needs a bolus reduction. Part 2 covers the 25/50/75% framework that Rabasa-Lhoret, Moser, West and Campbell have developed for this.
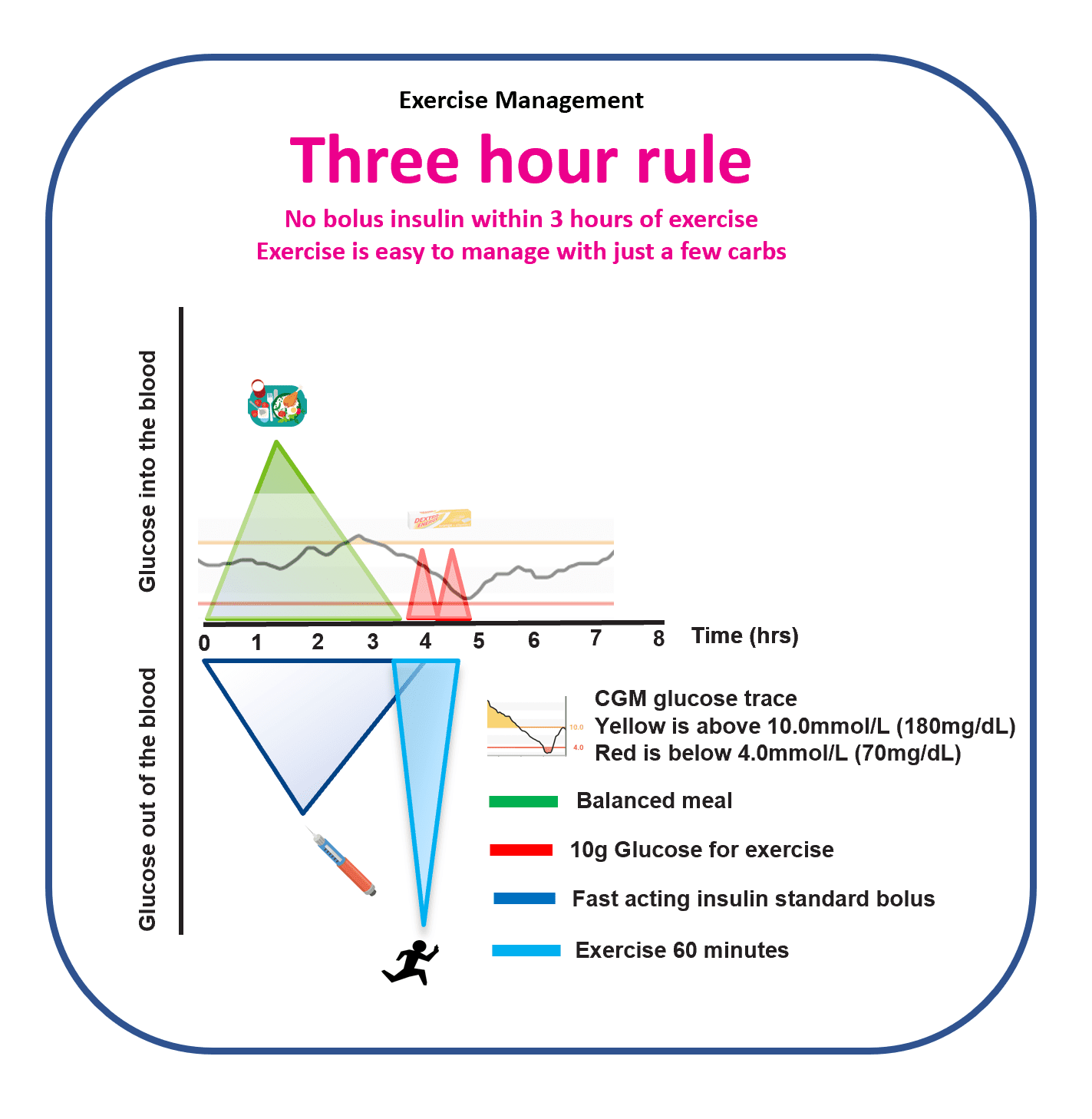
The Three-Hour Rule
One heuristic simplifies exercise management more than almost any other. When the last bolus was at least three hours before exercise, glucose behaviour is often far more predictable. Insulin on board has fallen, peak action has passed, and the exercise effect is less likely to be amplified into a fast drop.
This is not a guarantee. It is an organising principle. Where possible, arranging exercise three hours or more after the last meal bolus tends to reduce hypos, corrections and mental load.
What GNL research shows
The GAME framework
Pemberton et al (2023, Pediatric Diabetes) set out the GAME framework (Glucose, Activity, Meal, Environment) as a way to make exercise decisions in paediatric T1D less reactive and more structured. The framework anchors the majors (IOB, starting glucose, trend) alongside the activity itself, the recent meal, and the context (heat, altitude, sleep). It is the foundation for the Dynamic Glucose Management approach that runs through the GNL explorers and the rest of this guide.
Exercise and CGM
CGM becomes less reliable during exercise. Sensor lag is real, movement artefacts happen, and rapid glucose change stretches the gap between interstitial and capillary glucose. Numbers during and immediately after exercise should be interpreted with a little more caution than usual. Part 5 covers the specific CGM-in-exercise evidence in more detail.
That said, CGM is still the single most useful tool for learning how your body responds to exercise. The goal is not to distrust the number. It is to read it alongside the trend and the context, and to iterate over weeks, not to chase every data point in the moment.
Explorers that pair with this Part
- 10, 20, 30 Minutes Walking to Lower Highs: the activity-snacking tool grounded in the physiology covered here.
- Carbs for 30 Minutes Exercise: operationalises the three majors and the 90-minute window.
- Planning for Before, During and After Exercise: the full planner that pulls all five Parts together.
This guide is educational. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The guide says contracting muscle takes up glucose through a pathway that does not need insulin. What is that mechanism, and why does it mean exercise lowers glucose even when very little insulin is around?
Reveal answer
Contracting muscle fibres move GLUT4 glucose transporters to the cell surface through calcium- and contraction-driven pathways that are largely insulin-independent (Sylow and colleagues describe this as the dominant pathway of exercise glucose uptake). Because this route does not require insulin, exercise lowers glucose even in near insulin-deficient states. On top of that, increased blood flow speeds absorption of insulin already present, so circulating insulin rises just as muscle is most sensitive to it. The take-home concept is that exercise supercharges the insulin already there rather than injecting more.
2Why does the guide say people with type 1 diabetes are disproportionately vulnerable to exercise-induced hypoglycaemia, compared with people without diabetes?
Reveal answer
In people without diabetes, the liver releases glucose (via glucagon and sympathetic drive) to match muscle demand during exercise. In type 1 diabetes the alpha-cell glucagon response is blunted (Colberg 2022), so this counter-regulation does not do its usual job. With muscle pulling glucose out rapidly and the normal defence weakened, the balance tips towards lows. This explains a population-level vulnerability; it is not a prediction for any one person, and exercise planning is a conversation for the care team.
3The guide says different exercise types tend to push glucose in different directions. What is the broad pattern for aerobic versus anaerobic exercise, and what mechanism drives the difference?
Reveal answer
Aerobic exercise (running, cycling, swimming) tends to lower glucose, because sustained muscle glucose uptake dominates. Anaerobic exercise (sprinting, heavy lifting) often raises it, because catecholamine and cortisol release push glucose out of the liver. Mixed or team sports can go either way depending on intensity balance and the insulin on board at the start. The three majors still decide the risk; exercise type tells you what direction to plan for. This is an average pattern to understand, not a rule that holds for every individual or session.
4Reducing insulin for exercise (MDI, pump, HCL)The more advanced lever, once the carb plan is familiar: 50/50/20 for injections and pumps, the temp-target framework for a hybrid closed loop
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The guide describes two levers for keeping glucose steady around exercise. What are they, and what decides which one you reach for?
2The 50/50/20 framework for injections and pumps and the temp-target framework for a hybrid closed loop use different reduction sizes. Why does the closed loop need smaller manual reductions?
3Everything in this section is described as a starting framework rather than a fixed dose. Why is that framing important?
The next lever: reducing insulin
Once the carbohydrate plan feels familiar, the second lever is reducing insulin. It is more advanced, because it changes your doses rather than adding food, and how you do it depends on how your insulin is delivered: multiple daily injections, a pump, or a hybrid closed loop. The frameworks below are population-average starting points to understand and explore with CGM and your care team, not personalised doses, and any change to insulin is a care-team decision.
The insulin-reduction lever on MDI and pump: the 50/50/20 framework
When exercise is planned around a meal, reducing that meal’s insulin is the lever that works with the physiology rather than against it. On multiple daily injections or a pump, a simple clinical teaching heuristic used in structured education is 50/50/20. It distils the graded, type-and-duration guidance (which ranges from about a 25% reduction for a short session up to about 75% for a long one) into one memorable rule to start from:
- 50% reduction to the pre-exercise meal bolus, when eating within about two hours before the session.
- 50% reduction to the meal bolus after exercise, because insulin sensitivity tends to be high in the hours that follow.
- 20 for the evening (exercise after 4 pm), as overnight protection, any one of: a 20% reduction to background basal insulin, or about 20 g of carbohydrate without fast-acting insulin, or about 20 g of protein.
It is a deliberate simplification: the fuller guidance grades the reduction by exercise type and duration, so a shorter or anaerobic session often needs less and a long aerobic one more. Treat 50/50/20 as a memorable starting point and refine the size with CGM and your care team, who own any change to insulin.
The insulin-reduction lever on hybrid closed loop: the temp-target framework
On a hybrid closed loop the algorithm does part of the work, so the manual reductions are smaller. T25/T25 is a simple teaching heuristic that distils the EASD/ISPAD 2025 AID-and-exercise consensus (Moser, Zaharieva, Pemberton) into two steps, keeping the loop in automatic mode throughout:
- T25 before: set a temporary higher target about 60 to 90 minutes before the session starts, and if eating within two hours before, reduce that meal bolus by about 25 to 33%.
- T25 after: return the target to normal, and reduce the next meal bolus by about 25 to 33%, while insulin sensitivity is still raised.
The consensus is clear that the loop should stay in automatic mode through exercise wherever possible, with the temporary higher target doing the work; disconnecting or switching to open loop is a last resort, not a default, because the algorithm’s basal reductions are part of what protects you during and after the session. Systems differ in how their exercise modes and temporary targets behave; the AID and exercise section below covers the device-specific detail.
Like 50/50/20, T25/T25 is a memorable simplification of a wider consensus range; the exact target and reduction are population-average starting points to observe through CGM, not personalised settings, and any change is made with your care team.
The exercise explorers
Each lever has a GNL explorer that lets you play with the population-average pattern for your own situation:
- Carbs for 30 Minutes Exercise, the exercise insulin-on-board calculator.
- Exercise Planning explorer, the full before, during and after planner.
- AID Algorithm Optimiser, for the device-specific lever logic on a closed loop.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The guide describes two levers for keeping glucose steady around exercise. What are they, and what decides which one you reach for?
Reveal answer
The two levers are carbohydrate and insulin reduction. Which one you reach for, and how much, depends on the three majors (insulin on board, starting glucose and trend), the timing of the session relative to food, and how insulin is delivered (multiple daily injections, a pump, or a hybrid closed loop). When there is enough active insulin that glucose is likely to fall, carbohydrate is the faster lever; when exercise is planned around a meal, reducing the meal insulin works with the physiology. These are population-average starting frameworks to understand, not personalised doses, and any insulin change is a care-team decision.
2The 50/50/20 framework for injections and pumps and the temp-target framework for a hybrid closed loop use different reduction sizes. Why does the closed loop need smaller manual reductions?
Reveal answer
On a hybrid closed loop the algorithm is already reducing or suspending basal insulin in response to falling glucose, and a temporary higher target set ahead of the session adds to that, so part of the work is automated. The manual reductions (about 25 to 33% to a pre-exercise meal bolus within two hours, and about 25 to 33% to the next meal bolus after, the T25/T25 framework) are therefore smaller than the 50/50/20 reductions used on injections or a pump, where there is no algorithm doing that part. The point to understand is that the same physiology is being managed, with the loop doing some of it. The numbers are population-average starting points, explored with CGM and the care team, not fixed settings.
3Everything in this section is described as a starting framework rather than a fixed dose. Why is that framing important?
Reveal answer
Because the response to a given amount of carbohydrate or insulin reduction varies considerably between individuals, and within the same person from day to day, depending on the type and intensity of exercise, the time of day, insulin on board and many other factors. A population-average framework is a sensible place to begin and a way of organising the decision; the personal pattern is learned over time with CGM data and the care team, who own any change to the personal plan. The frameworks teach the shape of the decision, not the answer for any individual.
5Activity snacking, and planning around a sessionShort repeated post-meal movement as a precision lever, plus the before / during / after planning frame (the one unique FAQ atom, folded in)
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The guide calls the 20-minute paradigm a reframe of an older default. What was the older default, and why does the guide argue the shorter version is more usable?
2Turner et al (2024) compared pre-dinner walking with post-dinner walking. What did they find, and what conclusion does the guide draw from it about a universal 'walk after every meal' rule?
3The guide cites the Via Negativa principle of trying behavioural levers before device levers. In the context of post-meal glucose, what does that look like in practice, and why is it framed this way?
4Planning a structured session is often framed as Before, During and After. At a conceptual level, what is each phase mainly concerned with?
The three majors still set the risk here; see Part 3.
Part 3 · Anchor thesis
Twenty minutes of moderate activity, timed into the postprandial window, can reshape a day.
The earlier default (“walk for 30 to 45 minutes after a meal to bring a high down”) is not wrong, but it is not practical. Most people do not have 45 minutes between meals. The 20-minute paradigm reframes post-meal activity as short, frequent, unexhausting and patterned. Walking pace, not a training session. Repeated across the day, not done once.
This Part draws together John’s research chain on activity between meals, the converging external evidence on sitting interruption, and the paediatric studies that anchor the broader literature. It is the flagship lever of this guide.
| at | before | drop | projected |
|---|---|---|---|
| 10 min | 9.8 | -2 | 7.8 |
| 20 min | 9.8 | -4 | 5.8 |
| 30 min | 9.8 | -6 | 3.8 |
| at | before | drop | projected |
|---|---|---|---|
| 10 min | 9.8 | -2 | 7.8 |
| 20 min | 9.8 | -4 | 5.8 |
| 30 min | 9.8 | -6 | 3.8 |
| at | before | drop | projected |
|---|---|---|---|
| 10 min | 9.8 | -2 | 7.8 |
| 20 min | 9.8 | -4 | 5.8 |
| 30 min | 9.8 | -6 | 3.8 |
| at | before | drop | projected |
|---|---|---|---|
| 10 min | 9.8 | -2 | 7.8 |
| 20 min | 9.8 | -4 | 5.8 |
| 30 min | 9.8 | -6 | 3.8 |
| at | before | drop | projected |
|---|---|---|---|
| 10 min | 9.8 | -2 | 7.8 |
| 20 min | 9.8 | -4 | 5.8 |
| 30 min | 9.8 | -6 | 3.8 |
What GNL research shows
The 20-minute paradigm: Pemberton 2024 and 2025
Pemberton et al (2024) examined physical activity as a tool to ameliorate postprandial hyperglycaemia in type 1 diabetes. Pemberton et al (2025) extended that into a paradigm reframe: short, repeated bouts of moderate activity in the post-meal window are often enough to blunt the postprandial peak without triggering a later hypo, provided insulin on board and trend direction are accounted for. Pemberton and Russon (2025) developed the underlying causal modelling that turns the paradigm from observation into a usable framework.
The four GNL papers together reframe activity from an all-or-nothing intervention into a precision tool dosed in minutes. The 10, 20, 30 Minutes Walking explorer operationalises the paradigm directly. The Activity Snacking pattern (twenty by two: twenty minutes, twice a day, after the two largest meals) is the simplest behavioural form of it.
Pre-meal versus post-meal walking
Turner et al (2024, Diabetes, Obesity and Metabolism) compared pre-dinner walks against post-dinner walks in adults with T1D. Pre-dinner walking produced greater time in range across the evening and overnight window than post-dinner walking of matched duration and intensity.
This does not mean post-meal activity is wrong. It means the default “walk after every meal” rule is not the only answer. Pre-meal activity primes muscle glucose uptake and insulin sensitivity ahead of the meal; a different mechanism from post-meal rescue. For some people, some meals, some times of day, pre-meal activity is the better lever. Match the activity to the pattern, rather than prescribing it as a universal post-meal rule.
Sitting is the signal
Prolonged sitting worsens postprandial glucose. This is one of the more robust findings across the activity-and-T1D literature.
- Campbell SIT LESS (2023): interrupting prolonged sitting with brief activity breaks reduces post-meal glucose excursions in T1D adults.
- Larsen (2024): frequent activity breaks during sitting produce lower postprandial glycaemia than continuous sitting.
- Seppala (2025): sedentary time independently associates with poorer glucose outcomes in T1D.
The take-away is not “exercise more”. It is “sit less, move more often”. The breaks can be a couple of minutes of walking every half hour or so. The evidence signal holds even at that dose. Engeroff et al (2023) added the post-supper walking arm of this same body of evidence: short walks after the evening meal blunt the late-day rise in a way that is easy to fold into normal life.
The paediatric evidence chain (the studies behind the paradigm)
The activity-between-meals story did not start with adults. The DirecNet-era studies established the baseline pattern that moderate exercise lowers glucose in paediatric T1D and carries a delayed overnight hypoglycaemia risk window.
- DIRECT (2005): girls on a treadmill, the foundational paediatric exercise-glucose study.
- Tansey (2006): moderate exercise in T1D youth, characterising the during- and post-exercise glucose response.
- Tsalikian (2006): exercise in T1D, anchoring the delayed overnight hypo window.
- Magulou (2023): postprandial glucose physiology specific to children and adolescents. Puberty brings insulin resistance and amplified post-meal excursions, which makes post-meal activity a particularly useful lever in this group.
- Riddell (2019, Pediatric Diabetes): quantifies the between-individual variation in exercise response. Even with matched conditions, adolescents differ substantially in how their glucose behaves. This is the headline argument for iterating with CGM rather than following a fixed rule.
These studies pre-date ubiquitous CGM but anchor the evidence base on which the 20-minute paradigm sits. Helleputte (2023) provides the systematic review of post-meal activity across the literature, drawing the threads together.
Why the peak matters: the cardiovascular case
Post-meal excursions are not only about chart aesthetics. Hanssen (2020) summarises the mechanistic and epidemiological links between postprandial hyperglycaemia and cardiovascular disease. Oxidative stress, endothelial dysfunction and glycation pathways all associate with excursion magnitude independent of mean glucose. Reducing the peak matters for long-term outcomes, not only for today’s time-in-range number.
This is the long-game reason to take the 20-minute paradigm seriously. The day-to-day reason is simpler: most people feel better when their post-meal curves are flatter, and the behavioural cost of a short walk is low.
Via Negativa
Try the behavioural levers before the device levers
Before reaching for a setting change, an algorithm tweak, or an extra bolus, try the behavioural levers first. Pre-bolus the next meal by ten to fifteen minutes and see what changes. Walk for ten minutes starting around the twenty-minute post-meal mark. Interrupt the next hour of sitting with a couple of minutes of movement every twenty minutes. Match the activity to the pattern; sometimes pre-meal beats post-meal. These cost nothing and can be tested in a single meal window. If they do not help, escalate to settings changes with the diabetes team.
What the evidence does not yet show
- Head-to-head randomised comparisons of the 20-minute paradigm against the older 30-45 minute default.
- Long-term (multi-year) outcomes of activity snacking on HbA1c, time-in-range, or complications.
- Reliable dose-response curves across age, insulin regimen, and AID system.
- The optimal timing window within “post-meal”: twenty minutes after, forty-five minutes after, or ride the rise.
These are live research questions. John’s ongoing work is contributing to the first two.
Explorers that pair with this Part
- 10, 20, 30 Minutes Walking to Lower Highs: the activity-snacking explorer built directly on the 20-minute paradigm.
- Planning for Before, During and After Exercise: the full planner that integrates activity snacking with the wider exercise framework.
This guide is educational. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The guide calls the 20-minute paradigm a reframe of an older default. What was the older default, and why does the guide argue the shorter version is more usable?
Reveal answer
The older default was ‘walk for 30 to 45 minutes after a meal to bring a high down’. The guide says this is not wrong but not practical, because most people do not have 45 minutes between meals. The 20-minute paradigm reframes post-meal activity as short, frequent, unexhausting and patterned (walking pace, repeated across the day, not done once). The claim, drawing on the Pemberton 2024 and 2025 work, is that short repeated bouts can blunt the post-meal peak without triggering a later hypo, provided insulin on board and trend direction are accounted for. It is a precision tool dosed in minutes, offered as a concept to explore with CGM.
2Turner et al (2024) compared pre-dinner walking with post-dinner walking. What did they find, and what conclusion does the guide draw from it about a universal 'walk after every meal' rule?
Reveal answer
Pre-dinner walking produced greater time in range across the evening and overnight window than post-dinner walking of matched duration and intensity. The guide is careful to say this does not make post-meal activity wrong; it means the default ‘walk after every meal’ rule is not the only answer. Pre-meal activity primes muscle glucose uptake and insulin sensitivity ahead of the meal, a different mechanism from post-meal rescue, so for some people, some meals and some times of day, pre-meal activity is the better lever. The point is to match the activity to the pattern rather than prescribe one universal rule.
3The guide cites the Via Negativa principle of trying behavioural levers before device levers. In the context of post-meal glucose, what does that look like in practice, and why is it framed this way?
Reveal answer
Before changing a pump setting, an algorithm parameter or adding an extra bolus, the guide suggests testing behavioural levers first: pre-bolusing the next meal by ten to fifteen minutes, walking for ten minutes from around the twenty-minute post-meal mark, and interrupting sitting with a couple of minutes of movement every twenty minutes. These cost nothing and can be tested in a single meal window; if they do not help, the next step is escalating to settings changes with the diabetes team. The framing is build-by-subtraction: try the simplest, lowest-risk lever before the more complex one. It describes general levers to explore, not personalised dosing.
4Planning a structured session is often framed as Before, During and After. At a conceptual level, what is each phase mainly concerned with?
Reveal answer
Before is mainly concerned with insulin on board (for example the Three-Hour Rule, where the last significant bolus is more than three hours before exercise, as a commonly used starting point). During is about staying in a sensible working range, checking glucose and trend regularly, and supplementing carbohydrate early and in small amounts rather than reacting to a low. After is about the risk windows that follow, the first one to two hours and, for some people, an overnight window after evening exercise. The aim is safe, repeatable plans that improve over time, not a perfect trace, and specific dose changes are worth discussing with the care team.
6AID and exerciseWhat automated insulin delivery can and cannot do, and why pre-planning still matters
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The guide's anchor claim is that AID 'does not remove exercise risk, it reshapes which lever you pull and when'. What is the asymmetry that makes pre-exercise planning still matter on an AID system?
2The guide lists what AID can and cannot do during exercise. Give two things it can do and two it cannot.
3The guide says the post-exercise window, not the during-exercise window, is the harder problem on AID. What is the evidence pattern behind that, and what does it imply for when planning ends?
The three majors still set the risk here; see Part 3.
Part 4 · Anchor thesis
AID does not remove exercise risk. It reshapes which lever you pull and when.
AID systems respond to glucose, not to effort. Exercise changes insulin sensitivity and glucose utilisation within minutes, but active insulin from recent meal boluses persists for hours. The algorithm can only reduce or suspend basal; it cannot recall insulin already on board. This is the IOB trade-off that sits behind every AID-plus-exercise decision.
What changes with AID is not whether the three majors matter, but how you respond to them. Announce strategies, temporary targets, exercise modes and pre-emptive carbohydrate sit on top of the same physiology Parts 1 to 3 cover.
The EASD/ISPAD 2025 consensus: the anchor
The EASD/ISPAD 2025 position statement (Moser, Zaharieva, Pemberton et al) is the Grade A reference for AID and exercise. It covers announced versus unannounced activity, temporary target increases, and per-system exercise modes for MiniMed 780G, Control-IQ, Omnipod 5, and CamAPS FX. Both lead authors are GNL Scientific Advisers, and the statement is the direct evidence base for the GNL Exercise Planning explorer.
The headline pattern from the consensus: announce planned exercise to the algorithm where possible, raise the target ahead of the session rather than during it, and accept that the post-exercise window is the harder problem rather than the during-exercise window.
The load-bearing idea is that a good plan spans Before, During and After rather than reacting in the moment: set up insulin on board ahead of time, supplement small and early during the session, then mind the recovery window once it ends.
Listen: Ep18, Othmar Moser. Exercise without fear, the Before-During-After playbook. Watch on YouTube or listen on Spotify.
What AID can and cannot do during exercise
What it can do
- Reduce or suspend basal insulin in response to falling glucose.
- Raise the algorithm target through an exercise mode or temporary target setting.
- Deliver micro-corrections automatically when glucose rises after exercise.
What it cannot do
- Recall bolus insulin already in subcutaneous tissue.
- Anticipate exercise the user has not announced.
- See the difference between aerobic and anaerobic effort; it sees only the resulting glucose.
- Override the physiology of the 90-minute window after a meal bolus.
The asymmetry is what makes pre-exercise planning still matter on AID. Reactive algorithm work is good. Proactive user input on top of it is better.
Announce strategies and the 30-minute activity feature
Zimmer (2023) reviewed announcement strategies across AID systems. Setting a temporary higher target or enabling exercise mode in advance of planned activity (typically a window of around an hour to ninety minutes ahead) reduces during-exercise hypoglycaemia. The exact ahead-of-time window varies by system and is one of the live calibration questions in the literature.
Turner et al (2024) examined Omnipod 5’s 30-minute activity feature specifically. The broader pattern across AID systems is that announce-ahead works better than reactive correction once exercise is under way.
The manual mode trade-off
Zaharieva (2023) and clinical experience converge on a real trade-off: many people find manual mode more predictable during specific exercise sessions because it removes the continuous background adjustments the algorithm makes. The cost is the loss of automated suspension if glucose drops unexpectedly. Many people use AID as the default and switch to manual or exercise mode only for specific session types where the algorithm’s responsiveness becomes a liability rather than an asset.
This is not a recommendation to switch to manual mode for every exercise session. It is acknowledgement that the algorithm-versus-manual choice is a real one, and that there is no universally correct answer.
Pre-emptive carbs and bolus reductions on AID
Zimmer (2023) and the EASD/ISPAD 2025 consensus both address the pre-exercise meal bolus question. For exercise planned within the 90-minute window after a meal, a meal bolus reduction in combination with the AID temporary target tends to balance hypoglycaemia prevention and post-exercise hyperglycaemia better than relying on the algorithm alone. The exact percentage reduction is the individualisation problem Part 2 covers in detail.
Tagougui (2020) provides the post-meal reductions evidence on AID specifically. The pattern across the literature is that smaller, earlier interventions outperform larger, later corrections.
Real-world AID and exercise: what the registries show
- Joubert (2025): real-world AID use indicates more variability around activity than pivotal trials reported. Expectations need calibrating accordingly.
- Wang (2024): paediatric AID and physical activity. Children using AID still see meaningful exercise glucose variation; the algorithm helps but does not flatten the response.
- Seckold (2025): three exercise types in adolescents on AID. Aerobic, anaerobic and mixed each produce different algorithm response patterns. The user still has to anticipate which type the session will be.
- Moser and Mader (2025): T1D camp data comparing MiniMed 780G and CamAPS FX (mylife) across multi-day sustained activity. One of the few direct between-system comparisons.
The post-exercise window is the harder problem
Two studies frame this clearly.
- Myette-Côté (2022): the one-to-two hour window after exercise remains a high-risk period for hypoglycaemia on AID, even when the during-exercise window is well-managed by the algorithm.
- Morrison (2022): late afternoon vigorous exercise on AID raises post-meal hypoglycaemia risk that evening, but does not necessarily raise overnight hypoglycaemia. The risk has shifted from overnight to post-exercise evening, rather than disappearing.
And looking further forward, Bergford (2023, T1DeXi) shows the next-day risk after long sessions is real and underappreciated. Long sessions leave elevated hypo risk into the following day, even after the session itself ends.
What GNL methodology adds
Treat AID-plus-exercise as a planning problem
GNL treats AID-plus-exercise as a planning problem rather than a reactive one. The Exercise Planning explorer operationalises the EASD/ISPAD 2025 consensus directly: choose the activity, time it relative to insulin on board, reduce the preceding meal bolus by a sensible starting amount if appropriate, engage the AID exercise mode or temporary target ahead of the session, and have fast-acting carbohydrate to hand. The AID Algorithm Optimiser explorer makes the underlying lever logic visible. The Activity and Exercise explorer simplifies the short-walk case that the research shows is almost always low risk and frequently effective.
Explorers that pair with this Part
- AID Algorithm Optimiser: explore the per-system levers (CF, AIT, ICR, Target) and see how they shape the algorithm response.
- Planning for Before, During and After Exercise: full planner built on the EASD/ISPAD 2025 consensus.
- 10, 20, 30 Minutes Walking to Lower Highs: the short-walk explorer that pairs with announce-ahead AID strategies.
- The IOB Trade-Off: how four AID systems handle IOB differently, including the Rakab 2025 finding that ultra-rapid insulin in AID produces less than 1pp TIR improvement. The exercise-specific IOB uplift (Leohr 2026) is reflected in all three GNL exercise explorers.
This guide is educational. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The guide's anchor claim is that AID 'does not remove exercise risk, it reshapes which lever you pull and when'. What is the asymmetry that makes pre-exercise planning still matter on an AID system?
Reveal answer
AID systems respond to glucose, not to effort, and they can reduce or suspend basal insulin but cannot recall insulin already on board from a recent meal bolus, which persists for hours. Exercise changes insulin sensitivity within minutes, so the algorithm is reacting to a fall it cannot fully prevent if there is significant active bolus insulin. That asymmetry, fast physiology plus un-recallable IOB versus a basal-only lever, is why proactive user input (announcing exercise, raising the target ahead of time, reducing a preceding bolus) still matters on top of the algorithm. This is a conceptual explanation, not a setting to copy.
2The guide lists what AID can and cannot do during exercise. Give two things it can do and two it cannot.
Reveal answer
Can do: reduce or suspend basal insulin in response to falling glucose; raise the algorithm target through an exercise mode or temporary target; deliver micro-corrections automatically when glucose rises after exercise. Cannot do: recall bolus insulin already in subcutaneous tissue; anticipate exercise the user has not announced; tell aerobic from anaerobic effort (it sees only the resulting glucose); override the physiology of the 90-minute window after a meal bolus. The lesson the guide draws is that reactive algorithm work is good but proactive user input on top of it is better. It describes how the technology behaves, not what any individual should set.
3The guide says the post-exercise window, not the during-exercise window, is the harder problem on AID. What is the evidence pattern behind that, and what does it imply for when planning ends?
Reveal answer
Myette-Côté (2022) found the one-to-two hour window after exercise stays a high-risk period for hypoglycaemia on AID even when the during-exercise window is well managed by the algorithm; Morrison (2022) found late-afternoon vigorous exercise raised post-meal hypoglycaemia risk that evening (risk shifting rather than disappearing); and T1DeXi data (Bergford 2023) show next-day risk after long sessions is real and underappreciated. The implication is that planning does not end when the session ends, the recovery window and sometimes the following day still carry risk. These are population-level findings to understand, and any change to AID settings is a care-team decision.
7Exercise, hormones and the female physiology gapSex-specific physiology the guidelines overlook: the menstrual cycle, fuel use, fasted exercise, menopause (Ep 33, Jane Yardley)
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The episode says exercise guidelines were largely built on male research, and that the late luteal phase changes insulin needs for many females. What pattern does it describe, and how is it framed?
2The episode argues that standard per-kilogram carbohydrate advice for exercise may overestimate a female's needs. What two physiological reasons does it give?
3The episode describes a fat-loss barrier specific to type 1 diabetes, and why fasted morning exercise is offered as a lever. What is the mechanism, and what makes fasted morning exercise favourable?
In this episode
Exercise guidelines for type 1 diabetes have been built predominantly on research conducted with male participants, yet females face distinct physiological challenges that standard recommendations do not address. Hormonal fluctuations across the menstrual cycle alter insulin requirements and fuel utilisation. Lower lean muscle mass changes carbohydrate needs during activity. High peripheral insulin levels create unique barriers to fat loss.
Professor Jane Yardley bridges the research gap between male and female exercise physiology. This conversation explores how menstrual cycle phases affect glucose management, why fasted exercise offers particular advantages for females with type 1 diabetes, how muscle and bone health in your twenties and thirties shapes functional mobility decades later, and why carbohydrate recommendations may systematically overestimate female athletes’ needs.
The female exercise physiology framework
- Menstrual cycle phases: Follicular phase (days 1-14, relatively stable glucose), periovulatory phase (days 13-15, individual variability), luteal phase (days 16-28, progesterone rises, insulin resistance tends to increase).
- Luteal phase insulin resistance: Affects approximately 60-70% of females with type 1 diabetes, typically lasting three to four days, with insulin needs increasing by 10-50% on average, but this varies significantly between individuals.
- Fuel utilisation differences: Females tend to use proportionally more fat as fuel during exercise compared to males, regardless of exercise type, oestrogen appears to promote fat oxidation.
- Body composition impact: Lower lean muscle mass in females means per-kilogram carbohydrate recommendations (e.g., 0.5-1.0 g/kg) likely overestimate needs.
- Peripheral hyperinsulinaemia barrier: Type 1 diabetes creates four to eight times higher peripheral insulin levels than normal physiology, this activates fat storage enzymes and suppresses fat release, making fat loss very difficult through calorie restriction alone.
- Fasted exercise advantage: Exercising before breakfast minimises insulin on board, promotes fat oxidation, reduces hypoglycaemia risk, and often requires no insulin adjustments.
- Muscle and bone health window: Peak muscle mass and bone density occur in the twenties and thirties, resistance training and weight-bearing activity during this period are associated with higher functional capacity and lower fracture risk later.
Key themes
1. The luteal phase tends to create predictable insulin resistance
Approximately 60-70% of females with type 1 diabetes experience increased insulin resistance in the late luteal phase (roughly days 22-28), driven by rising progesterone. This typically lasts three to four days and, on a population-average basis, can increase total daily insulin requirements by roughly 10-50%, with significant individual variability; this is a population pattern, not a personal target, and any change to insulin is a decision made with your diabetes care team. AID systems were not designed to account for menstrual cycles and often struggle to keep pace with this shift.
2. Exercising in the luteal phase may require different insulin strategies
Physical activity increases insulin sensitivity, but during the luteal phase, basal rates are often already elevated to compensate for progesterone-driven insulin resistance. The same exercise at the same time of day may require different insulin management strategies depending on menstrual cycle phase, this is worth exploring with your care team and your own CGM data.
3. Females tend to use more fat as fuel during exercise
Research in people without diabetes consistently shows that females oxidise proportionally more fat during exercise compared to males, regardless of exercise intensity or type. This appears to be mediated by oestrogen. If females are relying more on fat oxidation and less on glucose oxidation, standard carbohydrate recommendations, largely derived from male-dominant studies, may overestimate needs.
4. Per-kilogram carbohydrate recommendations likely overestimate female needs
Standard exercise carbohydrate guidance does not account for sex-based differences in body composition. On average, females have higher body fat percentage and lower lean muscle mass. Since muscles are the primary consumers of glucose during exercise, a 70 kg female has less metabolically active tissue than a 70 kg male, meaning the same per-kilogram prescription may overestimate her carbohydrate needs.
5. Peripheral hyperinsulinaemia creates a fat loss barrier in type 1 diabetes
Insulin delivered subcutaneously bypasses the liver and enters peripheral circulation, resulting in four to eight times higher insulin levels in muscle and fat tissue compared to physiological delivery. High peripheral insulin activates fat storage while suppressing fat release; this helps explain why, as a physiological mechanism, calorie restriction alone tends to be an unsustainable strategy for fat loss in type 1 diabetes. This is educational mechanism, not a diet or weight-loss plan; any change to eating or activity for weight is a conversation with your care team.
6. Fasted morning exercise creates conditions for fat oxidation
Exercising before breakfast, with no bolus insulin on board for eight or more hours, creates the metabolic conditions for fat oxidation. Morning fasted exercise is associated with no insulin on board from meal boluses, elevated cortisol and growth hormone that promote fat as a fuel source, minimal hypoglycaemia risk, and no need for insulin adjustments in many cases.
7. Bolus insulin lasts longer than standard teaching suggests
The standard teaching that rapid-acting insulin peaks at two hours and is done by three to four hours significantly underestimates the actual duration of action. In practice, bolus insulin has a tail that extends up to six hours, particularly for larger doses, which has implications for exercise timing and hypoglycaemia risk throughout the day.
8. Fasted exercise depletes glycogen and tends to improve all-day insulin sensitivity
Beyond the immediate effects during exercise, fasted morning activity depletes muscle and liver glycogen stores, creating a metabolic state that may improve insulin sensitivity for the rest of the day. This effect tends to be particularly relevant for people with high total daily doses.
9. Building muscle and bone in your twenties and thirties shapes health decades later
Peak muscle mass and peak bone density occur in the twenties and thirties. The rate of decline in muscle strength, bone density, and functional mobility tends to be faster in females with type 1 diabetes compared to males with type 1 diabetes or the general population. The intervention window is early adulthood, not retirement.
10. Menopause brings insulin need changes and accelerated health risks
Perimenopause creates unpredictable glucose patterns as oestrogen and progesterone fluctuate. Post-menopause, insulin needs generally decrease. Cardiovascular risk increases sharply in females with type 1 diabetes after menopause, and loss of muscle mass and bone density accelerates, underlining the importance of maintaining physical fitness throughout the lifespan.
11. Pregnancy exercise data are limited but general principles are clear
Pregnancy with type 1 diabetes carries higher risks. In the general population, physical activity during pregnancy reduces complications, but robust data on safe, effective exercise protocols for type 1 diabetes pregnancy are limited. Reducing sedentary time, walking regularly (especially after meals), and maintaining as much activity as safely possible are the physiologically sound starting points. Always discuss exercise plans during pregnancy with your diabetes and obstetric teams.
Practical exploration checklist
General principles across the menstrual cycle
- Track your menstrual cycle and note patterns in glucose management, insulin needs, and exercise responses
- Expect individual variability, not all females experience luteal phase insulin resistance, and those who do vary in severity
- Test the same exercise in different cycle phases to identify your personal patterns
- Your CGM data is the most useful tool for exploring where you sit on the distribution
Fasted morning exercise, possible advantages to explore
- Exercise before breakfast, before the first bolus of the day
- Start with no insulin adjustments, many people find they can exercise fasted without changing basal rates or targets
- Suitable for moderate-intensity aerobic exercise and resistance training
- Discuss with your care team before making changes to your management routine
Carbohydrate intake during exercise, a starting point for exploration
- Standard recommendations may overestimate female needs due to lower lean muscle mass and higher fat oxidation
- Start with less than recommended and adjust based on actual glucose response
- For fasted morning exercise, you may need little or no carbohydrate supplementation
Building muscle and bone health
- Incorporate resistance training two to three times per week (weightlifting, bodyweight exercises, resistance bands)
- Include weight-bearing activities: walking, jogging, dancing, jumping
- After age thirty, shift focus to maintaining the peak you have built
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Listen: Ep33, Jane Yardley. Exercise, hormones and the female physiology gap. Watch on YouTube or listen on Spotify.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The episode says exercise guidelines were largely built on male research, and that the late luteal phase changes insulin needs for many females. What pattern does it describe, and how is it framed?
Reveal answer
Roughly 60 to 70 percent of females with type 1 diabetes experience increased insulin resistance in the late luteal phase (about days 22 to 28), driven by rising progesterone. It typically lasts three to four days and, on a population-average basis, can raise total daily insulin requirement by about 10 to 50 percent, with wide individual variability; this is a population pattern, not a personal dose, and any insulin change is made with the care team. AID systems were not designed around the menstrual cycle and can struggle to keep pace. This is a population-level pattern to recognise, not a personalised dose: the way to find your own pattern is to track the cycle alongside your CGM and explore it with your care team.
2The episode argues that standard per-kilogram carbohydrate advice for exercise may overestimate a female's needs. What two physiological reasons does it give?
Reveal answer
First, females tend to oxidise proportionally more fat (and less glucose) during exercise, an effect attributed to oestrogen, so they draw less on carbohydrate at a given intensity. Second, on average females carry a higher body-fat percentage and lower lean muscle mass, and muscle is the primary consumer of glucose during exercise, so a 70 kg female has less metabolically active tissue than a 70 kg male. Because the standard per-kilogram figures came largely from male-dominant studies, the same prescription may overestimate her carbohydrate needs. It is offered as a reason to start lower and observe the CGM response, not a fixed rule, and changes are explored with the care team.
3The episode describes a fat-loss barrier specific to type 1 diabetes, and why fasted morning exercise is offered as a lever. What is the mechanism, and what makes fasted morning exercise favourable?
Reveal answer
Insulin delivered subcutaneously bypasses the liver and reaches peripheral tissue at roughly four to eight times physiological levels; this high peripheral insulin activates fat storage and suppresses fat release, which is why calorie restriction alone is an unsustainable fat-loss strategy in type 1 diabetes. Exercising before breakfast, with no meal bolus on board for eight or more hours and with cortisol and growth hormone promoting fat as fuel, creates conditions for fat oxidation with minimal hypoglycaemia risk and, for many people, no insulin adjustment needed. These are population-level mechanisms to understand and explore with CGM and the care team, not instructions to change a regimen. The same caution applies more strongly in pregnancy, where exercise data in type 1 diabetes are limited and any plan is made with both the diabetes and obstetric teams.
8Take the exercise-response model apart (M7)Mastery is appraisal, not more tips: where the type-and-intensity model holds, where individual variation dominates, and how good the evidence is (CGM-accuracy caveats, T1DeXi, Syno/MIMIC, altitude, when to ask the care team)
Check yourself first
Can you answer these yet? If you are not sure, read the section below. If you are already confident, jump straight to the answers and compare.
1The first tactic is to treat CGM accuracy during exercise as conditional. Why is CGM less reliable during exercise, and what practical reading habit does the guide recommend as a result?
2The guide treats the Syno/MIMIC Lab dataset as confirming several real-world patterns. What does it say about where the largest time-in-range gain from daily steps occurs, and what is the equity implication?
3The closing tactic is 'when to ask your care team'. What does the guide say is the point at which the levers in the guide stop being enough, and how does it describe the role of the guide itself?
Mastery · Take the model apart
Where the model holds, where individual variation takes over, and how good the evidence is
The earlier sections covered the mechanism, the levers, the post-meal paradigm and AID. Mastery is not more tips: it is holding the same facts to a higher standard of appraisal. The points below are where the type-and-intensity response model holds, where individual variation dominates, and how strong the evidence actually is, drawn across registries, real-world AID datasets, sex differences and altitude. Each is a way of judging the evidence and your own pattern with a diabetes team, not a rule.
Treat CGM accuracy during exercise as conditional
CGM is the most useful tool for learning how your body responds to exercise. It is also less accurate during exercise than at rest. Sensor lag, movement artefacts and rapid glucose change all stretch the gap between interstitial and capillary glucose.
The practical rule is to read the number alongside the trend arrow and the context, and to be slower to react to a single reading mid-session. Iterate over weeks, not within a session.
Sex differences are real and underappreciated
Yardley (2023), Heyman (2025) and the wider literature on sex differences in exercise response in T1D point in a consistent direction: glucose response to matched exercise differs across the menstrual cycle and between sexes more than the older literature suggested.
The practical implication is not a separate set of rules, but an explicit acknowledgement that the same session on different days of the cycle can behave quite differently; and that this is signal rather than noise. Tracking the pattern over a few cycles often reveals it.
Fear of hypoglycaemia is a planning variable
Patton (2024) and the broader literature on fear of hypoglycaemia in T1D consistently identify it as one of the largest barriers to regular exercise. The fear is reasonable. The cost of avoiding exercise because of it is usually larger than the cost of the hypo it is trying to prevent.
Practical mitigation rather than dismissal is the useful framing. A rehearsed hypo response, fast-acting carbohydrate within reach, an exercise plan made in advance with the diabetes team, and CGM alarms set sensibly: all reduce the cognitive cost of starting the session.
Barriers and facilitators matter as much as physiology
Garcia (2024) and Johansen (2024) characterise the barriers and facilitators to physical activity in T1D. Time, fear, lack of structured support, and the cognitive load of exercise planning all rank highly. Facilitators include peer support, structured programmes, and clear practical guidance from the diabetes team.
The implication for an individual is that the right exercise plan is one that fits the rest of life. The most evidence-based session you cannot actually do is worse than a less optimal one you can repeat for years.
Altitude changes the rules
Altitude affects glucose metabolism, insulin sensitivity and CGM accuracy in ways the lowland literature does not fully cover.
The practical pattern many people find is that the first few days at altitude often need different settings from sea level, and that exercise responses can be amplified or blunted depending on intensity and acclimatisation. Plan altitude trips with the diabetes team rather than improvising on arrival.
Muscle damage and creatine kinase
Dial (2021) examined the relationship between exercise-induced muscle damage and insulin sensitivity in T1D. Heavy eccentric work (long downhill runs, novel resistance training, certain team sports) can produce a multi-day pattern of altered insulin sensitivity that does not match the immediate post-exercise window most planning frameworks focus on.
The signal here is that the day of an unfamiliar or eccentric session is not the only day that matters. The two or three days that follow may need their own adjustments.
T1DeXi shows the real-world pattern
The T1DeXi dataset and its follow-on analyses (Bergford 2023; T1DeXi adolescents 2024) provide one of the largest real-world exercise-and-T1D evidence bases now available. Two patterns stand out.
- Hypo risk on exercise days is meaningfully higher than on non-exercise days, and the risk extends into the following day after long sessions.
- Real-world exercise produces more variable glucose response than pivotal trials of the same protocols. The trial average is a starting point, not a forecast for any individual.
Calibrate expectations to the registry data, not to the clinical-trial average.
What GNL research shows
Syno and MIMIC Lab insights
The Syno/MIMIC Lab dataset (Stanford, 667 users, 373,737 patient-days; analysed April 2026, a primary-study subset of the GNL programme of approximately 1,300 people and approximately 500,000 patient-days) confirms several patterns that the smaller trial literature only suggested.
- Exercise improves time-in-range, but the effect is modest and varies by AID status. AID users gain a little more than non-AID users.
- The largest TIR gain from daily steps occurs between zero and around five thousand steps. Above that, incremental gains diminish sharply. Getting sedentary people moving matters more than pushing already-active people further.
- Hypoglycaemia risk rises with exercise duration and varies by intensity and type; strength training appears to be the safest type for hypo risk in this cohort.
- Long sessions (over an hour) leave elevated hypo risk into the following day. The session itself is not where the planning ends.
- Higher correction-bolus frequency on AID does not associate with increased time-below-range. The automated suspension does its job.
These findings underwrite the structure of the GNL explorers and the heuristics through this guide.
When to ask your care team
This guide is education, not prescription. The point at which the levers in this guide stop being enough is the point to bring your diabetes team in. That includes, but is not limited to, recurrent unexplained exercise hypoglycaemia, post-exercise hyperglycaemia that does not resolve, new exercise types or intensities that change the pattern significantly, pregnancy, altitude trips, and any change to insulin regimen or AID system.
The role of this guide is to make the conversation with the care team a more structured one: to bring the patterns and the questions, rather than the raw chaos of a difficult week.
Explorers that pair with this Part
- Planning for Before, During and After Exercise: the full planner that integrates all five Parts.
- 10, 20, 30 Minutes Walking to Lower Highs: the activity-snacking explorer.
- Carbs for 30 Minutes Exercise: the exercise IOB calculator.
- AID Algorithm Optimiser: for the AID-specific lever logic.
This guide is educational. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Answers · check yourself
Reveal each answer and compare it with what you thought. When you can answer them, mark the guide as read.
1The first tactic is to treat CGM accuracy during exercise as conditional. Why is CGM less reliable during exercise, and what practical reading habit does the guide recommend as a result?
Reveal answer
Sensor lag, movement artefacts and rapid glucose change all stretch the gap between interstitial and capillary glucose, so a CGM reading during exercise can trail the true value. The recommended habit is to read the number alongside the trend arrow and the context, to be slower to react to any single mid-session reading, and to iterate over weeks rather than chasing each data point within a session. The deeper point is epistemic humility about the measurement itself, which is a Mastery-level appraisal skill rather than a fixed instruction.
2The guide treats the Syno/MIMIC Lab dataset as confirming several real-world patterns. What does it say about where the largest time-in-range gain from daily steps occurs, and what is the equity implication?
Reveal answer
The largest share of the time-in-range gain from daily steps occurs between roughly zero and about five thousand steps; the gain is modest in size, and above five thousand steps the incremental gains diminish sharply. The implication the guide draws is that getting sedentary people moving matters more than pushing already-active people further. It is framed as a population-level pattern (667 users and 373,737 patient-days in the GNL primary-study subset of this dataset) that should calibrate expectations and priorities, not as a personal step target; individual response varies and exercise plans are made with the care team.
3The closing tactic is 'when to ask your care team'. What does the guide say is the point at which the levers in the guide stop being enough, and how does it describe the role of the guide itself?
Reveal answer
The point to bring in the diabetes team is when the levers in the guide stop being enough: examples given include recurrent unexplained exercise hypoglycaemia, post-exercise hyperglycaemia that does not resolve, new exercise types or intensities that significantly change the pattern, pregnancy, altitude trips, and any change to insulin regimen or AID system. The guide describes its own role as making the conversation with the care team more structured, bringing the patterns and questions rather than the raw chaos of a difficult week. It is explicit that it is education, not prescription.
Exercise is not random. It is fast physiology meeting slow insulin. The climb runs from what exercise is and the three majors, through the mechanism, the insulin and carb levers, activity snacking and AID, up to taking the exercise-response model apart and weighing how good the evidence is.
This content is for educational exploration only. It describes average responses and general principles, including working GNL frameworks (heuristics to experiment from) that are starting points, not rules. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team. Any change to insulin doses or settings is a decision for you and your care team.
GNL Exercise hub · Foundations → Advanced → Mastery · serves G8 + M7