Foundations, Part 1
What is Type 1 Diabetes?
A diagnosis often arrives in a fortnight: thirsty all the time, going to the loo at night, weight dropping off, a strange smell on the breath. A finger-prick reads high, a blood ketone reads higher, and the words “type 1” land in a room that until that morning had nothing to do with diabetes. The first thing to know is that the body’s machinery has not failed at random; a specific part of it has stopped working, and from now on something else has to do that job.
The part of the body that has stopped working
The pancreas sits behind the stomach. Inside it are small clusters of cells called the islets of Langerhans, and inside those islets are beta cells, the cells that make insulin. In type 1 diabetes the immune system, which normally fights infection, mistakenly identifies these beta cells as foreign and removes them. Over months or years, beta cell numbers fall to the point where the body cannot produce enough insulin to keep glucose in a workable range. By the time symptoms appear, most of the working beta cells are already gone (Atkinson et al, The Lancet, 2014).
This is autoimmune, not lifestyle. It is not caused by eating too much sugar, by being overweight, or by anything a person did or did not do before diagnosis. The triggers that set the autoimmune process in motion are still under research; the mechanism, immune-mediated loss of insulin-producing cells, is settled.
Why insulin is essential, not optional
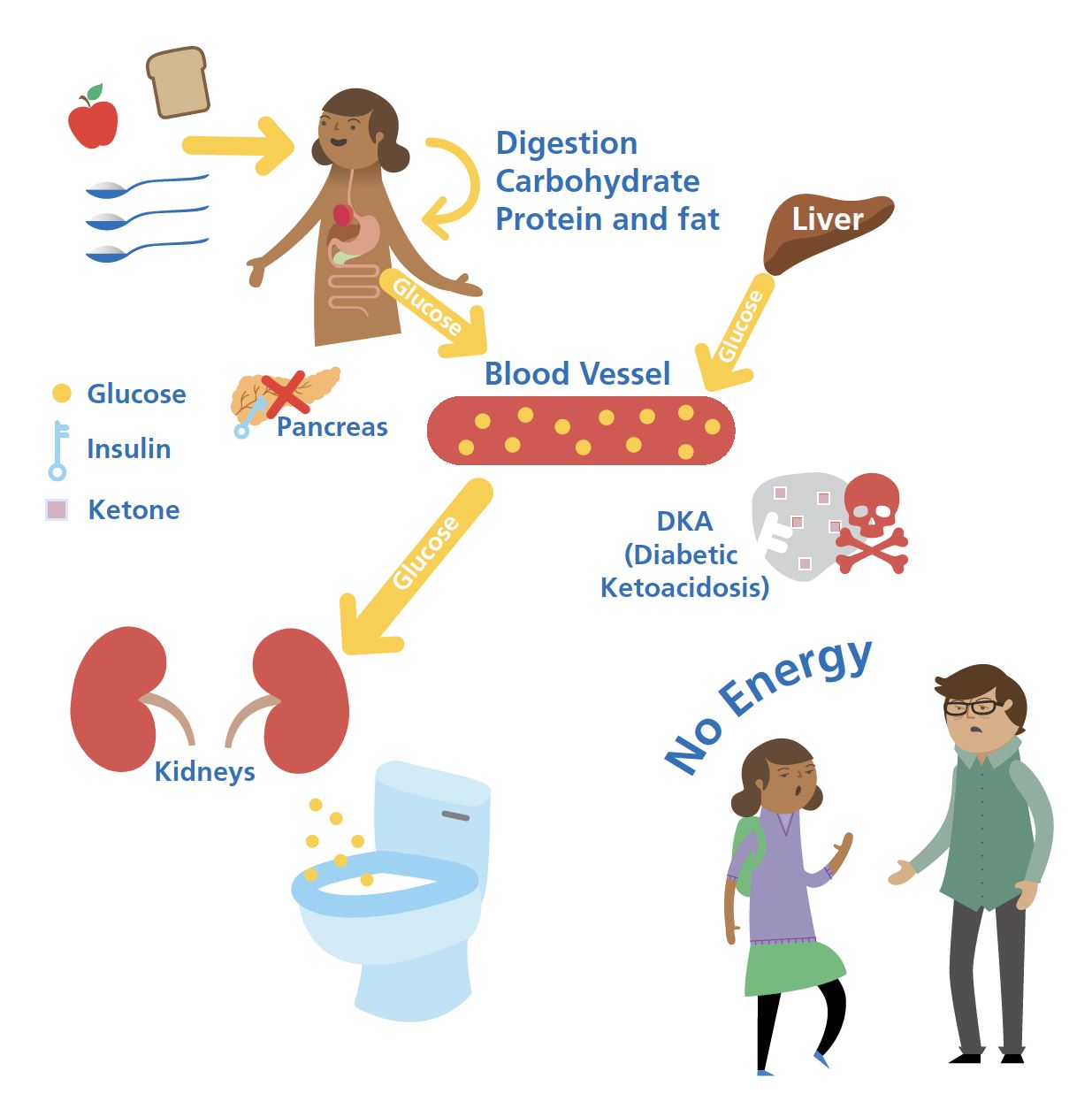
Insulin is the signal that lets glucose move from the bloodstream into muscle, fat, and liver cells, where it is used for energy or stored for later. Without insulin, glucose stays in the bloodstream and rises; the body then breaks down fat for fuel, which produces ketones. High glucose plus rising ketones is diabetic ketoacidosis (DKA), a medical emergency.
For someone living with type 1 diabetes, insulin is not a treatment that makes things better. It is the missing signal that has to be replaced, every day, for life. Pumps deliver it continuously through a small cannula under the skin. Pens deliver it as injections at meals and once or twice a day for background cover. The job is the same in both cases: to put insulin into the body in roughly the right amount at roughly the right time, and to learn from what happens next.
The job, stated plainly. A working pancreas adjusts insulin every few seconds based on glucose, exercise, food, illness, and stress. Type 1 diabetes asks the person and their tools to do that job from outside the loop. The Foundations guide is the working knowledge that makes the job manageable.
What changes after diagnosis
Three things shift on the day of diagnosis, and they keep shifting for months afterwards.
Glucose becomes a number that has to be checked. A working pancreas knows the glucose level continuously and adjusts. After diagnosis, the person has to know it instead, and act on it. Continuous glucose monitoring (CGM) is the tool that makes this possible without finger-pricks every couple of hours. Foundations Part 2 explores how it works and why it underpins everything else in this guide.
Food becomes information. Not a moral category, not a list of allowed and forbidden things, but information. Carbohydrate has the largest, fastest effect on glucose; understanding how much is in a meal is what lets a bolus dose be matched to it. Foundations Parts 6 and 7 cover this without the diet-culture overlay.
Daily life enters the loop. Sleep, stress, exercise, illness, hormones, alcohol: each of these moves glucose through different mechanisms and on different timescales. Most people do not realise how much these things mattered until type 1 diabetes makes them visible.
The honeymoon, and what comes after
For a few months after diagnosis, the remaining beta cells often produce a small amount of insulin. This is the honeymoon period. Glucose tends to behave better than it will later, and insulin doses are typically lower. The honeymoon ends gradually, not all at once, and the body’s own contribution falls toward zero over the following one to three years on average. The implication is straightforward: insulin doses will need to rise as the honeymoon fades, and what worked in the first six months will need to be revisited. This is normal physiology, not a sign that something has gone wrong.
This page is for educational exploration only. It describes general patterns and accepted clinical understanding. It is not medical advice and cannot replace individual guidance from your diabetes care team.
Part 1 of 12
What is Type 1 Diabetes?