Part 1, infants and preschoolers
Infants and preschoolers with T1D (under 6)
2am, the room lit by the CGM. The trace is climbing, the dose you would give in daylight is a fraction of a unit, and the smallness of it is what makes you pause. The youngest body cannot tell you it feels low or high. You learn to read what it can say.
The way the diagnosis arrives
You may not have been told there was any reason to look. The cot felt damp at 4am, the appetite shifted, the nappies changed weight, the breathing went a little faster, and by the time anyone in a uniform said the word “ketoacidosis” the child was already in trouble. From the conversations I have with families in clinic, what parents describe is the same shape in almost every case. The textbook was written for older children, and infants present with vomiting, sleepiness, and faster breathing first.
The largest international study we have on this set the pattern down honestly (Cherubini 2020, Diabetologia). Across 13 countries and approximately 59,000 newly diagnosed children, around 60 percent of babies diagnosed under their first birthday arrived in DKA. Across the whole under-5 band the figure sat at around 35 percent. The under-1s peak is consistent across countries, the ethnic-minority and lower-HDI signal is consistent across countries, and the trend has not improved over a decade of public-awareness campaigns alone.
The harder line in the Cherubini paper is the trajectory: the rate did not improve over the eleven years of follow-up, and rose slightly in some countries. The pattern crosses country borders, sits more heavily in children from ethnic-minority backgrounds, and tracks inversely with the country’s overall Human Development Index. None of those facts implicate any individual family; they describe a health-system signal that is everyone’s problem and no individual’s fault.
The textbook signs of T1D, the polyuria-polydipsia-weight-loss triad and the fruity breath, were written for children who can tell you they are thirsty and old enough to wet the bed at night when they were not the night before. Infants present differently. Vomiting, sleepiness, faster breathing, fewer wet nappies that all look about right because the toddler is a toddler. The signal that something has changed is often a feeling more than a fact: she is not herself, the milk is not going down, the cot is too quiet at the wrong time of day. Parents are usually right when they have that feeling; the system around them is not always set up to act on it before the bloods are drawn.
If a baby in your family is unwell in a way that is not behaving like the usual viral picture, the four signs to ask about by name are thirst, weight loss, more wet nappies, and faster breathing. The conversation with the GP or out-of-hours team is a finger-prick glucose, framed as a worry rather than a request. It takes less than five minutes and rules T1D in or out on the spot.
The case for screening before the crisis
There is a quieter version of this story, told by families who never reached A&E in an ambulance. They knew their child was at higher genetic risk; they had a phone number, a three-monthly check, and a name on a clinic letter for when the antibodies first turned positive. By the time their child needed insulin, the family was watching for it.
The clearest evidence on what that does sits in the TEDDY follow-up (Elding-Larsson 2011, Diabetes Care). Children screened from infancy and followed every three months presented in DKA at diagnosis at 15 percent in the under-2 band, against 39 to 54 percent in the matched national registries with no screening pathway. Severe DKA, the pH-under-7.1 group, fell with it. The difference is not pharmacological. It is structural: the family already knows what to watch for, the child is already being seen every three months, and the OGTT and antibody tracks identify Stage 3 onset before the crisis.
Two reframes follow from that. The first is that the under-1s peak is not biology being unkind; it is a system that is not seeing infants soon enough. The second is that the gap between 15 percent and 54 percent is the size of effect that awareness plus structured follow-up can carry, before any insulin, any device, or any change in clinical practice. In the UK the general-population screening question is moving slowly; ELSA, INNODIA Stage 2 pathways, and the early-T1D NICE consideration are the threads to watch.
For a family that already has T1D in the room, a first-degree relative screen is a conversation worth opening with the diabetes team, framed as a question about siblings rather than a diagnostic claim. The team will know which UK pathway fits.
The dose is small, the work is yours
After the first admission, the picture in the cot changes shape but not weight. The dose is small enough that a 0.1-unit error matters. The child cannot tell you they feel low. The CGM line at 4am becomes the closest thing to a voice they have. Mealtimes shift, illness scrambles the basal pattern, growth spurts pull insulin needs in directions no spreadsheet predicts. The day-to-day variability in this age group is structural, not behavioural. It is one of the reasons modern guidance has moved toward systems that can respond faster than a parent at the bedside can.
Two trials reshaped what is possible in this age group. In KidsAP02 (Ware 2022, NEJM), children aged 1 to 7 on CamAPS FX gained around 8.7 percentage points of time in range over 16 weeks, equivalent to roughly 2 hours a day, with nighttime time in range reaching 82 percent and no severe hypoglycaemia or DKA across the trial. In the Omnipod 5 preschool single-arm evaluation (Sherr 2022, Diabetes Care), 2 to 5.9 year-olds added around 10.9 percentage points of time in range, HbA1c fell by approximately 0.55 percent over 13 weeks, and there were no severe hypoglycaemia or DKA events. Different system, similar direction of effect.
What the trials describe, and what families in clinic describe, is the same shift in where the work goes. The algorithm carries the overnight basal work; the parent picks up the carbohydrate-counting at meals, the change of pod or set, the school or nursery conversation, and the noticing that an off day is on its way. The systems do not remove the work. They move it. For many families that means more sleep, fewer 3am corrections done by hand, and the cognitive space to be a parent first and a basal-trace reader second.
None of this is easy to start, and access varies by country, by integrated-care board, and by family circumstance. Your paediatric diabetes team is the first conversation. Ask early, ask in writing if you need to, ask again if the first answer is “not yet”.
Tight is safer than it used to be
For a long time the conversation in clinic, on the parent forums, and in the older literature was that pushing tight in the youngest age group cost you in hypoglycaemia and in family burnout. The fear of a low at the bottom of the cot drove targets upward; the parents who watched the most carefully often did the highest variability work for the smallest glycaemic gain. It is a fair description of an earlier era of care.
The Swedish national-register picture, summarised by Sundberg 2025 (Diabetes Care), is the cleanest counter-evidence available. In children under 7 with modern care (CGM in 96 percent, pump in 89 percent, AID increasingly), an HbA1c below 6.5 percent (48 mmol/mol) sat in 42 percent of the cohort in 2023. Tight-range time (3.9 to 7.8 mmol/L, 70 to 140 mg/dL) above 50 percent has held steady at 51 to 55 percent of the national cohort since 2019. Severe hypoglycaemia rates have not risen with the tighter targets, and the cohort’s weight has not climbed. The 2024 ISPAD preschool chapter (Ch23) carries the same framing forward: tighter glycaemic targets are achievable safely in this age band where families have access to the modern toolkit and an experienced diabetes team.
What modern care can safely deliver in under-5s on AID plus CGM. Sundberg’s Swedish registry shows tight-range time above 50 percent in roughly half the national under-7 cohort, with no rise in severe hypoglycaemia or weight. The same data carry the warning that sits underneath: DKA risk on AID concentrates at higher HbA1c bands, with the increased risk most visible at HbA1c 7.5 percent or above and pronounced at 8.5 percent and above (Karges 2024, Lancet Diabetes Endocrinol). The benefit and the safety case both depend on the team behind the device.
The pivot for a family weighing all of this is that the conversation is no longer about whether AID can help in the youngest age band; it is about timing, access, training, and the team. The team makes the device useful; the device alone does not.
The Dusk-Then-Drop pattern
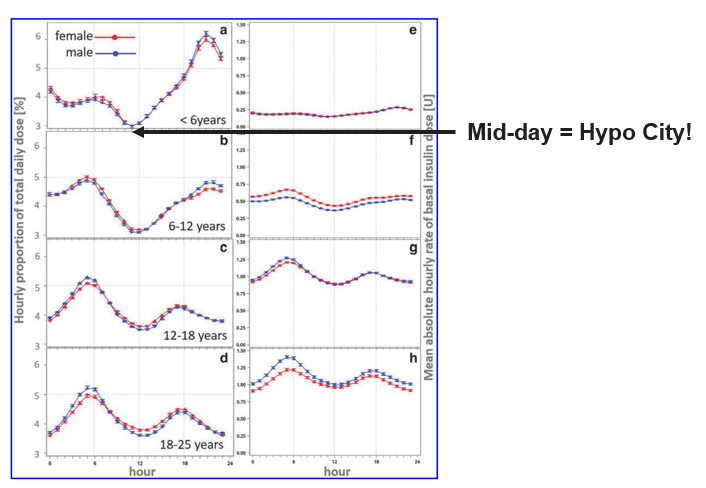
From the conversations I have with families running AID in this age band, one pattern comes up again and again. The dinner-time line lifts off around 17:00 and keeps lifting through to 22:00, then the moment the household goes to sleep the line tips the other way and the overnight risk shifts from hyper to hypo. Parents learn to recognise the shape before they have a name for it. The DPV registry data carry the structural reason: children under six show the most distinct diurnal pattern of any paediatric age group, with a clear evening rise in insulin need and an overnight fall (Biester et al. 2023, Diabetes Technology and Therapeutics, DPV registry, n=25,718 young people on CSII; ISPAD 2024 chapter 23), and the early-evening rise compounded by an overnight fall is the band’s signature.
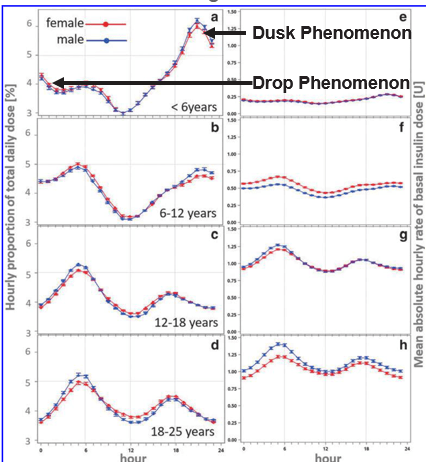
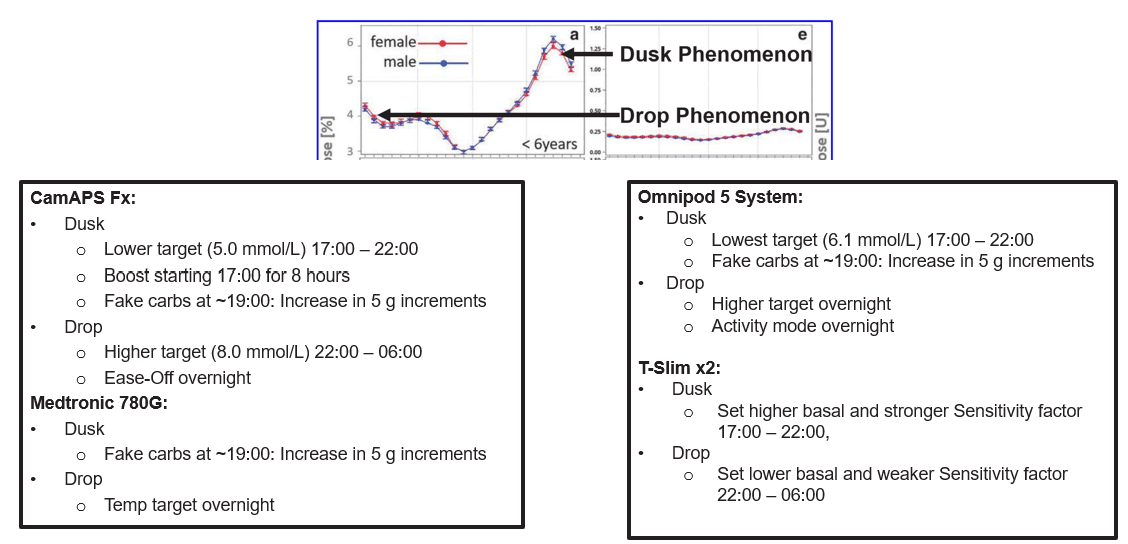
The clinic conversation that follows from this pattern has three levers, each tied to an AID system and each a discussion to have with the team rather than a setting to change alone. Some teams trial a stronger correction factor or a lower target through the dusk window; some trial a small, planned bolus around 19:00 to break a stubborn rise; some run a weaker correction factor or a higher target through the overnight window to keep the algorithm from over-delivering once resistance drops. The shapes of those conversations are different by system, and the picture below holds the three current systems side by side.
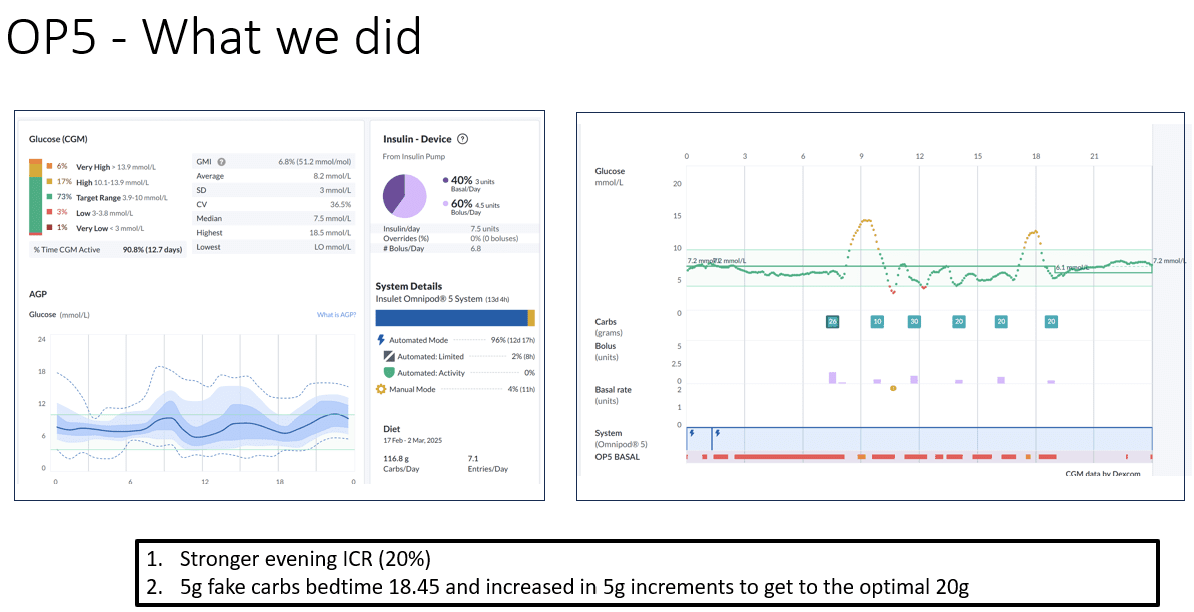
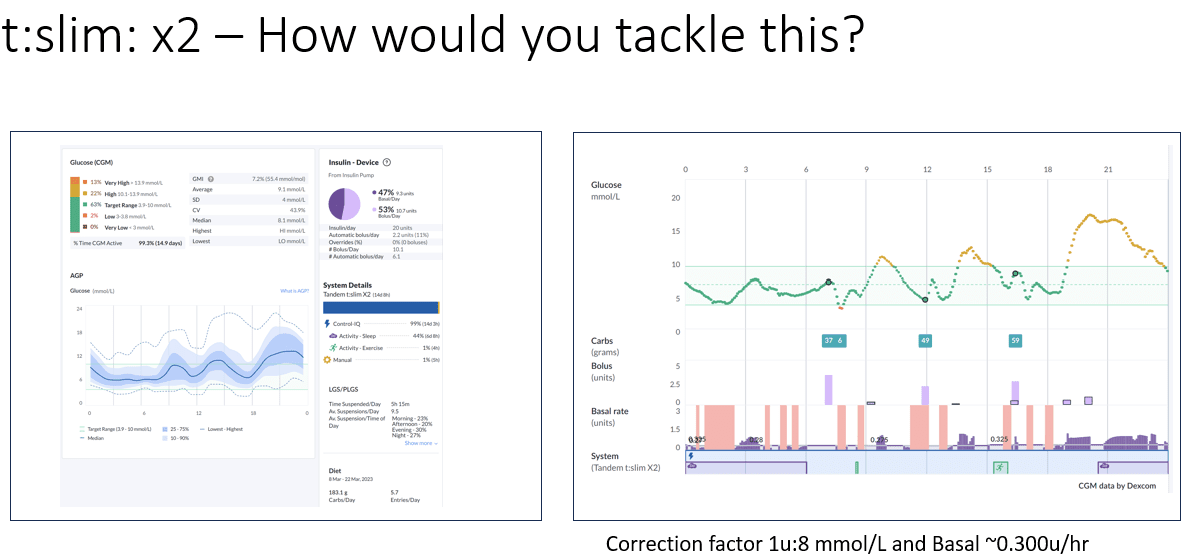
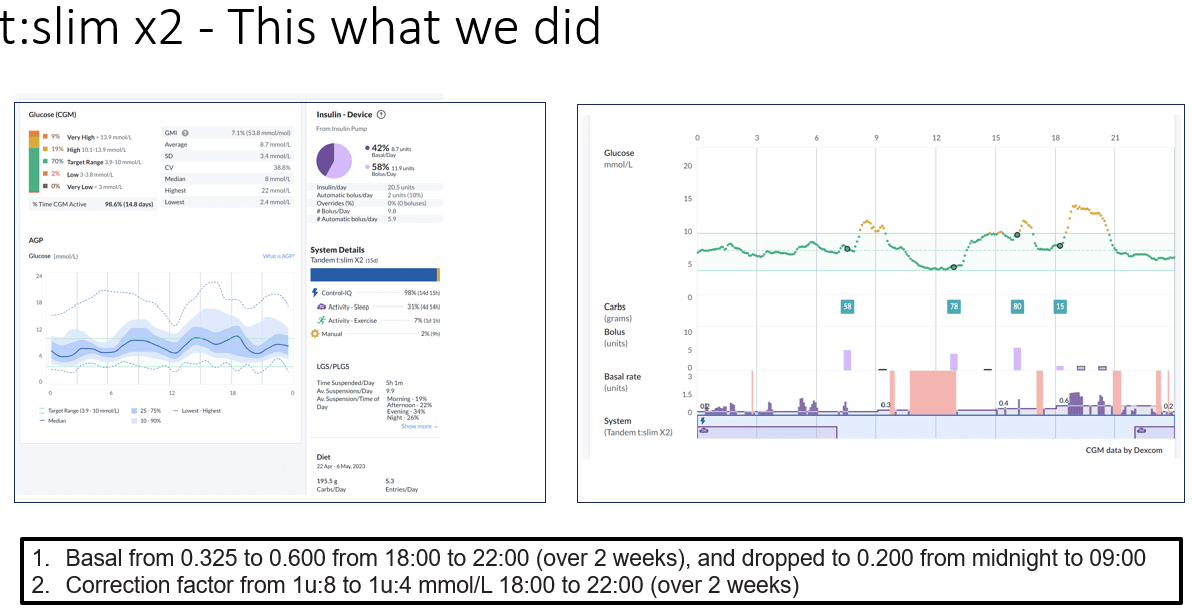
The graphic below holds the three system-specific levers in one frame so the family can see the shape of the conversation before they sit down with the team. The numbers are population-average starting points anchored to TDD; the personal correction factor your child uses, the actual basal pattern, and the actual target are settings the diabetes team owns. People have their own correction factors set with their care team. The picture is the conversation opener, not the dose.
The aim is not zero spikes. The aim is fewer evenings that run away, and fewer nights where insulin is stuck high after the dusk phase ends. The conversation in clinic is the route through.
The midday hypo trap
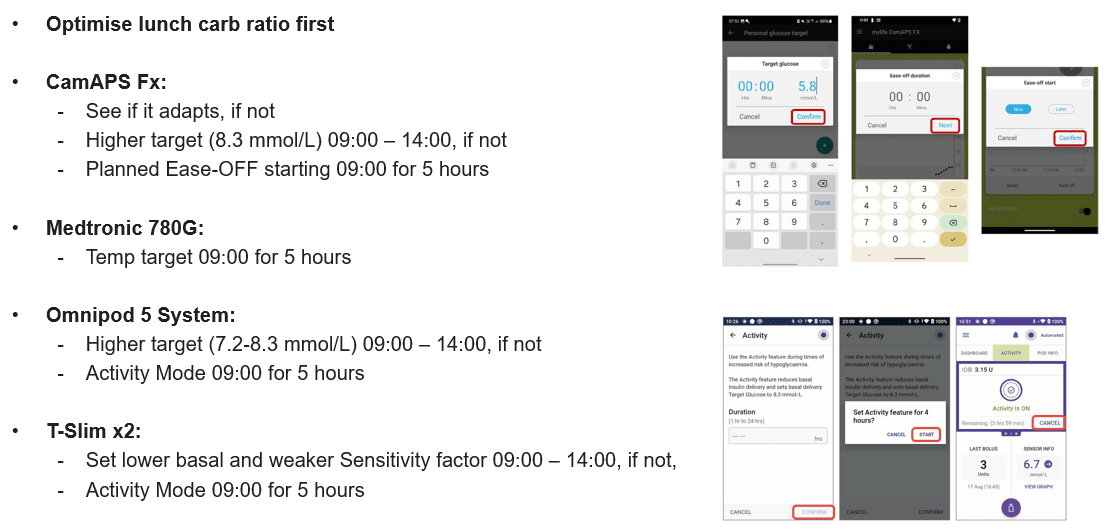
The flip side of the dusk-then-drop pattern, in many under-6 families, is the window between 11:00 and 14:00. The mood drops; the playground goes quiet ten minutes earlier than usual; the line on the CGM is heading down before the lunch bolus has cleared. For many children in this age band, the period around and after lunch is one of higher insulin sensitivity than the breakfast or evening window. That is the structural cause; the parent’s translation system is what catches it.
The lever many paediatric teams use to start the conversation is the meal-specific insulin-to-carb ratio. From the conversations I have in clinic, the rules of thumb anchored on total daily dose are population-average starting points, not personal prescriptions: roughly 150 divided by TDD as a breakfast ratio, roughly 250 divided by TDD at lunch (the weakest, because sensitivity is highest), and roughly 200 divided by TDD in the evening. The figures are the shape of the conversation, not the dose; people have their own meal-specific ratios set with their diabetes care team based on TDD, the child’s pattern across recent weeks, exercise and growth and illness context, and other factors. If a parent does not know their child’s current ratios, the figures here should not be used to set them; the team is the conversation.
What the figures describe is the direction the paediatric clinic moves toward when a child shows the midday-trap pattern. Stronger at breakfast, weaker at lunch, moderate in the evening. The aim is fewer midday lows and fewer rebound corrections that drive the early-afternoon line up later. The diabetes team will set the actual ratios.
Pre-bolusing the toddler who has not decided about lunch yet
A toddler is the worst piece of evidence the family has on whether the lunch the parent has just laid out will be eaten. The dose-first-eat-later school of pre-bolusing works beautifully for a six-year-old who knows their own appetite; it collapses the moment a two-year-old looks at the plate, says “no”, and slides off the chair. Most teams I work with recommend a stepped ladder for the families building confidence with pre-meal dosing in this band.
The stepped pre-bolus ladder
- Start with around 50 percent of the meal bolus delivered 5 to 15 minutes before food, with the remainder given once the parent has seen what the child will actually eat.
- Move to around 75 percent up-front once the child’s appetite pattern is more predictable and the post-meal CGM line is consistently in range.
- Build towards a full pre-meal bolus, around 15 minutes ahead, when the predictability is there and the team agrees the spike control is worth the carry.
The percentages are starting points the team will refine for the child in front of them; carbohydrate counting accurate to within 5 to 7 grams is what makes the maths land at the smallest doses.
The pivot is recognising that pre-bolusing is a tool the family grows into, not a step everyone in this band can take from week one. The team will know where the child sits on that ladder and when to ask for more.
When the dose is under five units
In the smallest children, total daily dose can sit below five units. At that scale, the resolution of an insulin pump or pen starts to argue with the maths; a 0.5-unit error on a 4-unit day is a tenth of the whole day’s insulin. From the clinic side, the conversations that come up here are about clinic-led tools that change the resolution: diluted insulin, where the team prepares insulin at a fraction of the usual concentration so the pump can deliver a meaningful fraction of a unit; or, on some systems, an Activity Mode setting around meals that adjusts the algorithm’s delivery for a planned window.
Neither of these is a parental adjustment. Diluted insulin is a paediatric specialist intervention that requires the team to prepare, label, and supervise the dilution and to retrain the family on the new units-on-display arithmetic. Activity Mode timing changes are settings the team helps set up and review. Where the dose is under five units, the conversation worth having with the team is whether the resolution problem is showing up in the data, and what the local service offers as a route through.
Routines and the second site of care
The biggest non-algorithmic lever in this age band is rarely a medical one. It is the rhythm of the day. Predictable mealtimes, predictable snacks, predictable sleep, predictable handoffs between caregivers. The variability in the under-6 day drives variability in the glucose. The behavioural literature most paediatric teams lean on for this is the Triple P (Positive Parenting Program) framework, which gives the structure for routines, calm setting limits, and shared responsibility across the household without making the diabetes the whole story of the child. A T1D-aware adaptation of the Triple P principles, delivered through the diabetes team or signposted by them, is what changes the rhythm of the day in practice.
The second site of care is where the rhythm has to travel. Nursery, grandparents, the babysitter on a Friday evening, the swim teacher. Every site needs a plan, a CGM-share permission, a glucagon rescue kit (nasal glucagon is licensed from age four and is materially easier for a non-clinician to deliver in a real emergency), and one clear point of contact. Most paediatric diabetes teams will help write the school or nursery plan if you ask. Ask your team for it; ask them to put it in writing; ask them to update it when the child moves between settings.
Nutrition sits alongside the rhythm. Schofield equations are the dietetic baseline for energy needs in growing children, and the team’s paediatric dietitian will use them as a starting point and adjust to growth, activity, and family context. A practical reference is around 40 to 50 percent of intake from carbohydrate in a balanced day, tuned to the child and the household. Carbohydrate counting accurate to within 5 to 7 grams is the resolution the under-5 doses need to land cleanly; small errors matter more when doses are tiny.
What carers tell us they need at home
The practical close in clinic is rarely a number. It is the things the family wants in place before the next nursery drop-off, the next bug going round the toddler group, the next holiday with the in-laws. From the conversations I have with families, the same handful comes up.
Ketone strips in the cupboard, the sick-day rule written down, and a number to ring out of hours. A nursery or childminder who has been taught what hypoglycaemia looks like at this age (quiet, pale, withdrawn, not the textbook tremor) and who has the carb treatment to hand. A second carer in the house who can do the overnight check without waking the household. A CGM share set up on more than one phone so the bedtime parent is not the only one watching. A list of “things that change the day” pinned somewhere visible, illness, growth spurt, big nap, big play, vaccination day, so the rise that arrives at 3pm has a name on it.
Hypoglycaemia treatment doses in this age band are weight-led, not the adult 15 g anchor. Your team will set the carbohydrate gram-per-kg starting point with you and revisit it. The GNL Hypo Treatment Explorer carries the band-appropriate framing and points you back to the team for the personal number. The aim is to walk into clinic with the question already shaped, not to substitute the explorer for the conversation.
The work is yours, and so is the right to keep asking for the tools that make it lighter. Particular thanks to Louise Collins, RN and Dr Ruth Krone at Birmingham Children’s Hospital, whose clinical practice shaped the under-5s patterns in this part.
Part 1 of 4
Infants and preschoolers with T1D (under 6)
Read more on GNL
References
Cherubini V, Grimsmann JM, Akesson K, et al. Temporal trends in diabetic ketoacidosis at diagnosis of paediatric type 1 diabetes between 2006 and 2016: results from 13 countries in three continents. Diabetologia. 2020;63(8):1530-1541.
Elding Larsson H, Vehik K, Bell R, et al. Reduced prevalence of diabetic ketoacidosis at diagnosis of type 1 diabetes in young children participating in longitudinal follow-up (TEDDY). Diabetes Care. 2011;34(11):2347-2352.
Glaser N, Barnett P, McCaslin I, et al. Risk factors for cerebral edema in children with diabetic ketoacidosis. New England Journal of Medicine. 2001;344(4):264-269.
Kuppermann N, Ghetti S, Schunk JE, et al. Clinical trial of fluid infusion rates for pediatric diabetic ketoacidosis (PECARN DKA FLUID). New England Journal of Medicine. 2018;378(24):2275-2287.
Ware J, Allen JM, Boughton CK, et al. Randomised trial of closed-loop control in very young children with type 1 diabetes (KidsAP02). New England Journal of Medicine. 2022;386(3):209-219.
Sherr JL, Bode BW, Forlenza GP, et al. Safety and glycaemic outcomes with a tubeless automated insulin delivery system in very young children with type 1 diabetes. Diabetes Care. 2022;45(8):1907-1910.
Karges B, Rosenbauer J, Stahl-Pehe A, et al. Hybrid closed-loop insulin therapy and risk of severe hypoglycaemia and diabetic ketoacidosis in young people (aged 2 to 20 years) with type 1 diabetes (DPV). Lancet Diabetes and Endocrinology. 2024.
Sundberg F, Smart CE, Samuelsson J, Akesson K, Krogvold L. Using time in tight glucose range as a health-promoting strategy in preschoolers with type 1 diabetes. Diabetes Care. 2025;48(1):6-14.
Sundberg F, deBeaufort C, Krogvold L, et al. ISPAD Clinical Practice Consensus Guidelines: managing diabetes in preschoolers. Pediatric Diabetes. 2024 update, chapter 23.
Biester T, Eckert A, Becker M, et al. Expected basal insulin requirement during continuous subcutaneous insulin infusion therapy by age group, sex, and body mass index, based on 25,718 young people with type 1 diabetes in the DPV registry. Diabetes Technology and Therapeutics. 2023;25(11):774-781. DOI: 10.1089/dia.2023.0283.
Sanders MR, Mazzucchelli TG, Studman LJ. Stepping Stones Triple P and the Positive Parenting Program for children with disability and chronic conditions. Behaviour Research and Therapy. (Triple P framework, paediatric T1D adaptation context.)
Schofield WN. Predicting basal metabolic rate, new standards and review of previous work. Human Nutrition: Clinical Nutrition. 1985;39 Suppl 1:5-41. (Schofield equations, dietetic baseline for paediatric energy needs.)
ISPAD Clinical Practice Consensus Guidelines 2024, chapters 11 (DKA), 12 (hypoglycaemia and insulin), 13 (sick day in paediatrics), 16 and 17 (technology), 23 (managing preschoolers). Pediatric Diabetes. 2024.