Hypoglycaemia: Foundations
Hypoglycaemia
Mid-morning, the CGM buzzes 3.9 mmol/L with the arrow tipping down. You reach for the glucose tablets, count four, swallow them with water, set the timer for twenty minutes. The dose, the wait, and what you reach for first are doing most of the work; the rest of this page explains why.
Ask Grace
Want to ask about treatment dose, impaired awareness, or how AID systems flatten the worst lows? Ask Grace.
What this page covers
- The treatment threshold: 4.0 mmol/L (70 mg/dL) is the standard action point, not the physiological definition of 3.3 mmol/L (60 mg/dL).
- Why pure glucose raises blood glucose within ten minutes when other carbohydrates take longer; and why glucose tablets are the most reliable delivery form.
- How body weight sets the dose: 0.3 g/kg capped at 60 kg, the paediatric figure from McTavish 2011 that ISPAD 2024 carries forward.
- Why sugar-based treatments tend to overshoot, and why the problem is dose stacking rather than the pharmacology of sucrose itself.
- What impaired awareness means (hypoglycaemia-associated autonomic failure, or HAAF), how AID systems cut the worst lows, and when glucagon rescue becomes the plan.
For the deeper three-part guide covering recognition, advanced treatment, and prevention strategies, see Part 1 on signs and nocturnal picture, then Part 2 on treatment protocols in depth, then Part 3 on prevention through basal review and IOB-aware corrections.
Video overview
This video walks through the key concepts covered on this page.
What glucose level counts as a hypo?
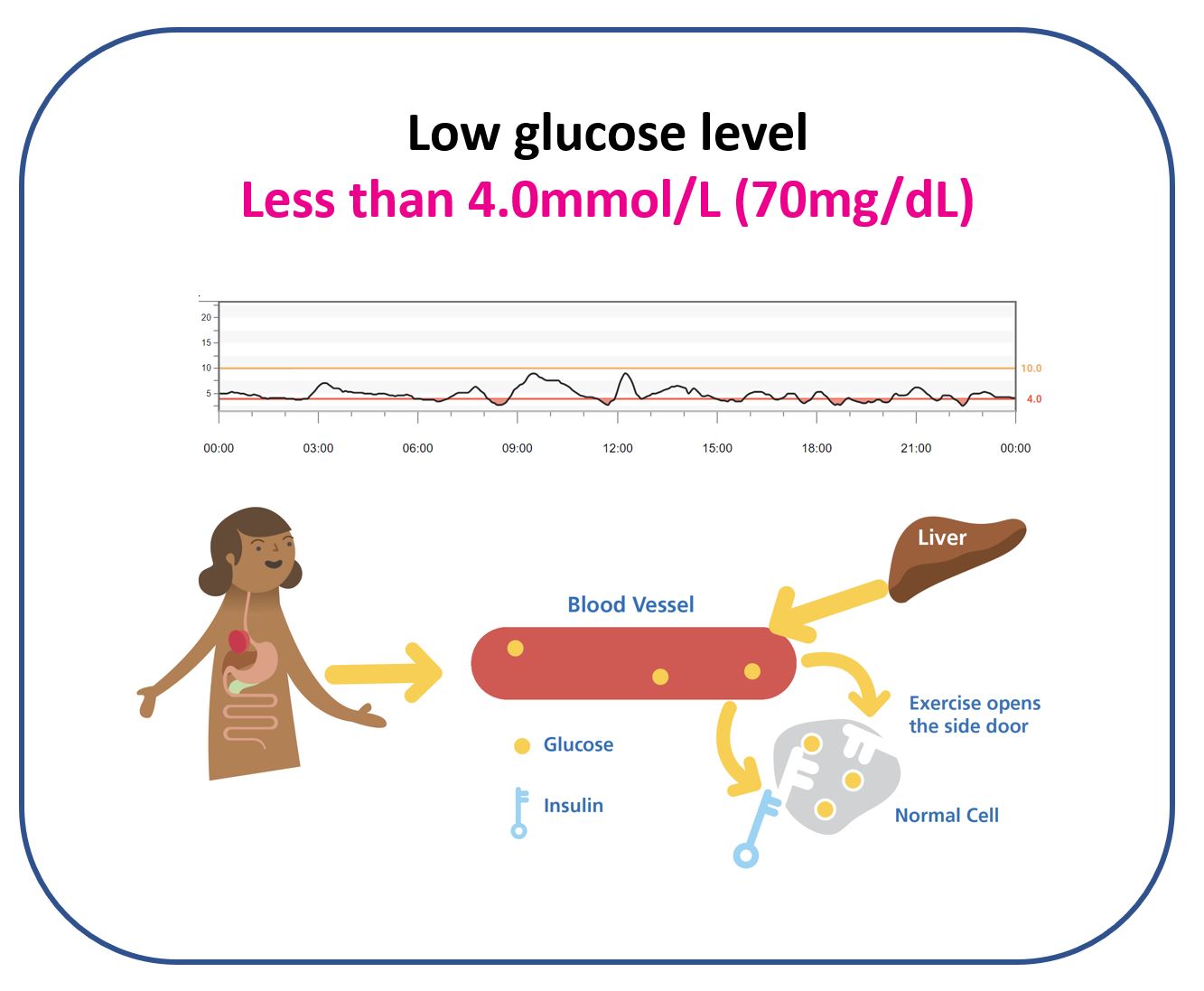
Physiologically, hypoglycaemia is a glucose level below 3.3 mmol/L (60 mg/dL). People without diabetes typically sit between 3.3 and 6.7 mmol/L (60 and 120 mg/dL) throughout the day.
In practice, 4.0 mmol/L (70 mg/dL) is the standard treatment threshold. In modern CGM accuracy studies, a reading in the low range is considered accurate if it falls within 0.8 mmol/L (15 mg/dL) of true blood glucose. If true glucose is 3.2 mmol/L (58 mg/dL), a CGM can read up to 0.8 mmol/L higher and still be labelled accurate. Setting the low alert at 4.0 mmol/L therefore tends to catch almost all true hypos before they become physiologically dangerous; setting it at 3.3 mmol/L can mask a true level near 2.6 mmol/L with no alarm.
Why pure glucose is the fastest treatment
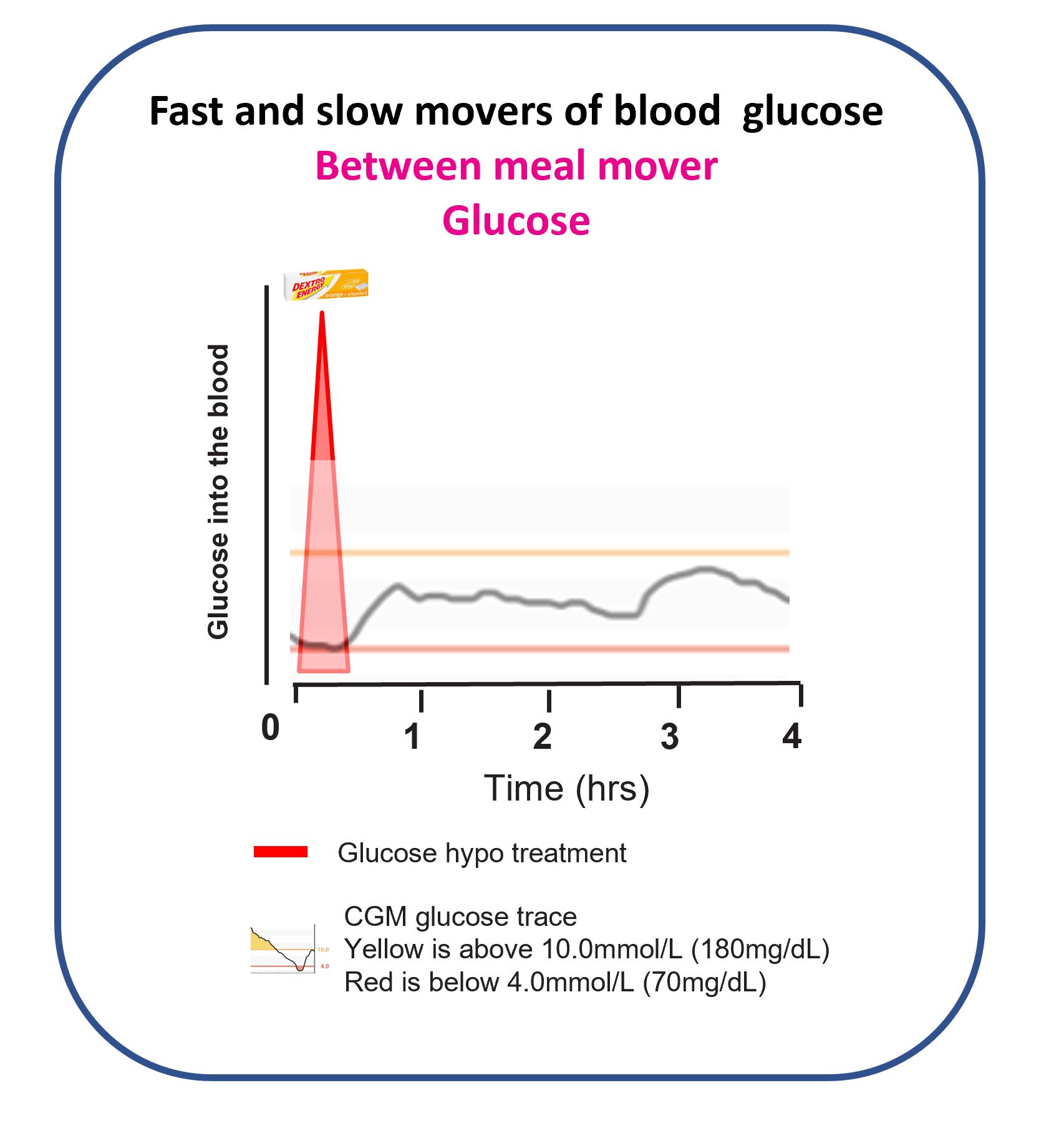
Pure glucose starts raising blood glucose in about ten minutes and has largely done its job by twenty. That is why the standard recheck point is twenty minutes, not five or ten.
Slama and colleagues (1990, 7-arm head-to-head crossover) tested glucose tablets, glucose solution, glucose gel, fruit juice, sucrose, and starch hydrolysate side by side in adults with insulin reactions. Glucose tablets produced the fastest rise; starch was the slowest; the others sat in the middle. That study underpins the “pure glucose first” framing across UK and ISPAD guidance.
Why body weight matters for dosing
Body weight is a rough proxy for blood volume and muscle mass. Larger bodies have more blood to fill with glucose and more tissue pulling glucose from the blood, especially after heavy bolus insulin or exercise. Treatment therefore tends to scale with weight.
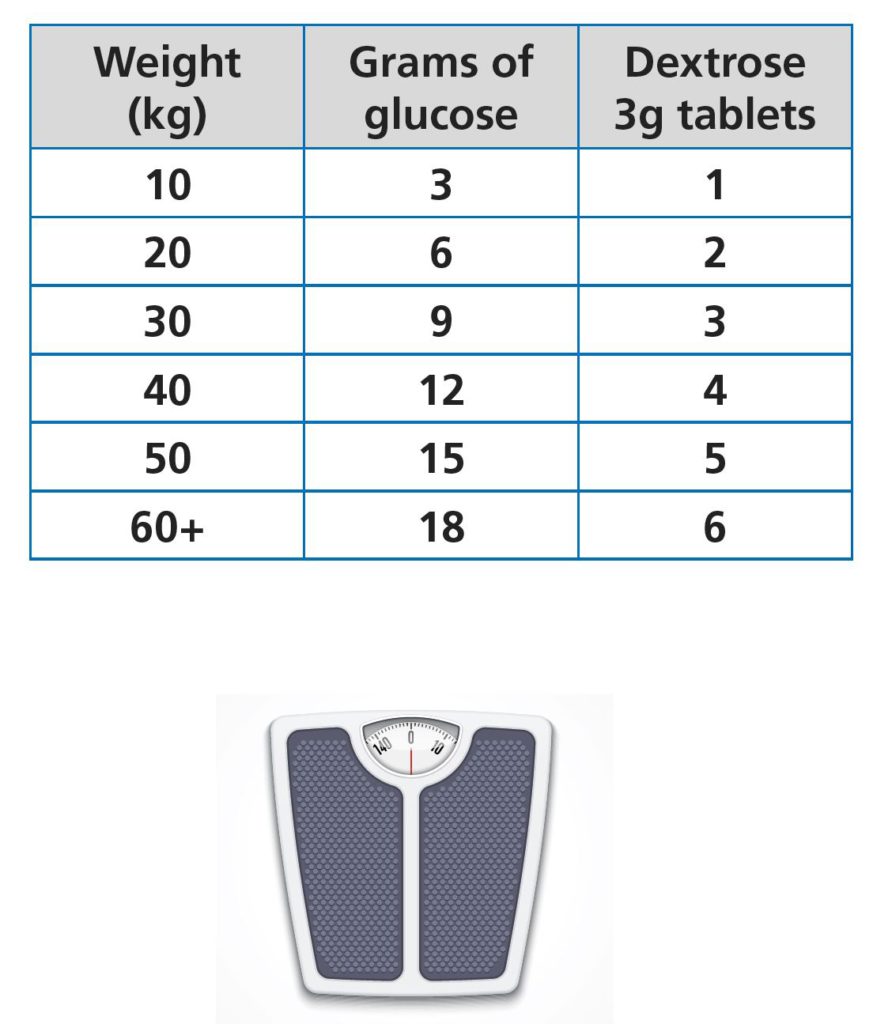
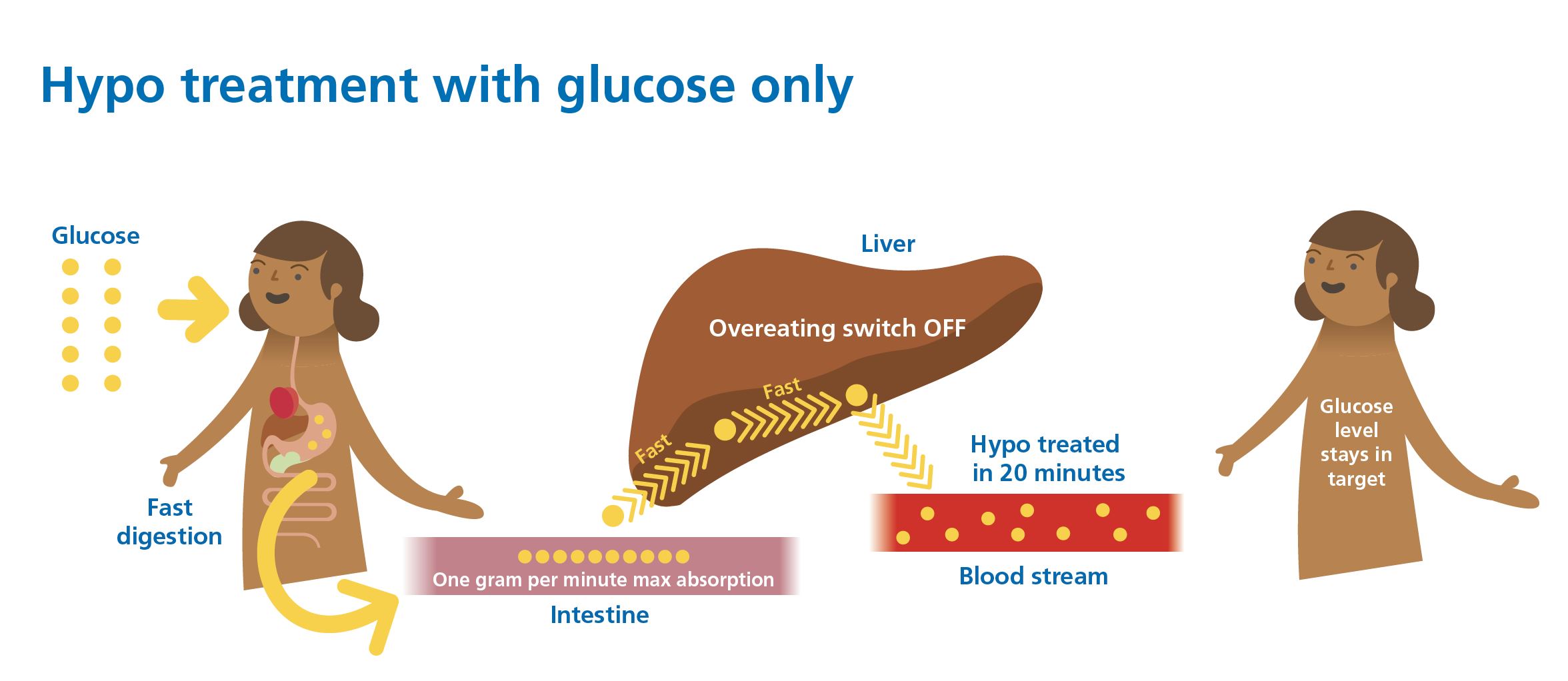
Weight scales the dose up to a 60 kg cap. Beyond 60 kg, a larger first dose does not land any faster; a second dose at the retest is the better answer than a single bigger dose that stacks in the gut. The intestine absorbs glucose at about 1 gram per minute via the SGLT1 single-source pathway, so the surfaced ceiling on the explorer sits at 18 grams (60 kg multiplied by the 0.30 g/kg paediatric ISPAD figure).
Weight-based dosing has trial support in McTavish and Wiltshire (2011, paediatric RCT, n=39), with 0.3 g/kg the most effective dose at the 15-minute recheck. ISPAD 2024 carries the figure forward with a reduce-to-5-to-10 g caveat in AID-era contexts to avoid rebound stacking.
Retest window with CGM lag. Recheck at 15 to 20 minutes if reading from a CGM (the CGM lags blood glucose by approximately 5 minutes); 15 minutes if finger-pricking. The wider window covers the lag and tends to avoid premature re-treatment that drives stacking.
Why glucose tablets tend to work best
- Cheap, portable, and stable (they do not go off).
- Small, consistent doses (usually 3 to 4 grams per tablet), easy to split for precision.
- Treating a hypo is medicine, not a snack. “Tasty treats” tend to blur that line and can drive overeating loops.
- Liquid “glucose” drinks (Lucozade, Gatorade, and similar) are messy: formulations change, some use mixed sugars, they are bulky, hard to measure precisely, and often expensive.
- For faster swallowing, many people find that taking glucose tablets with water works well.
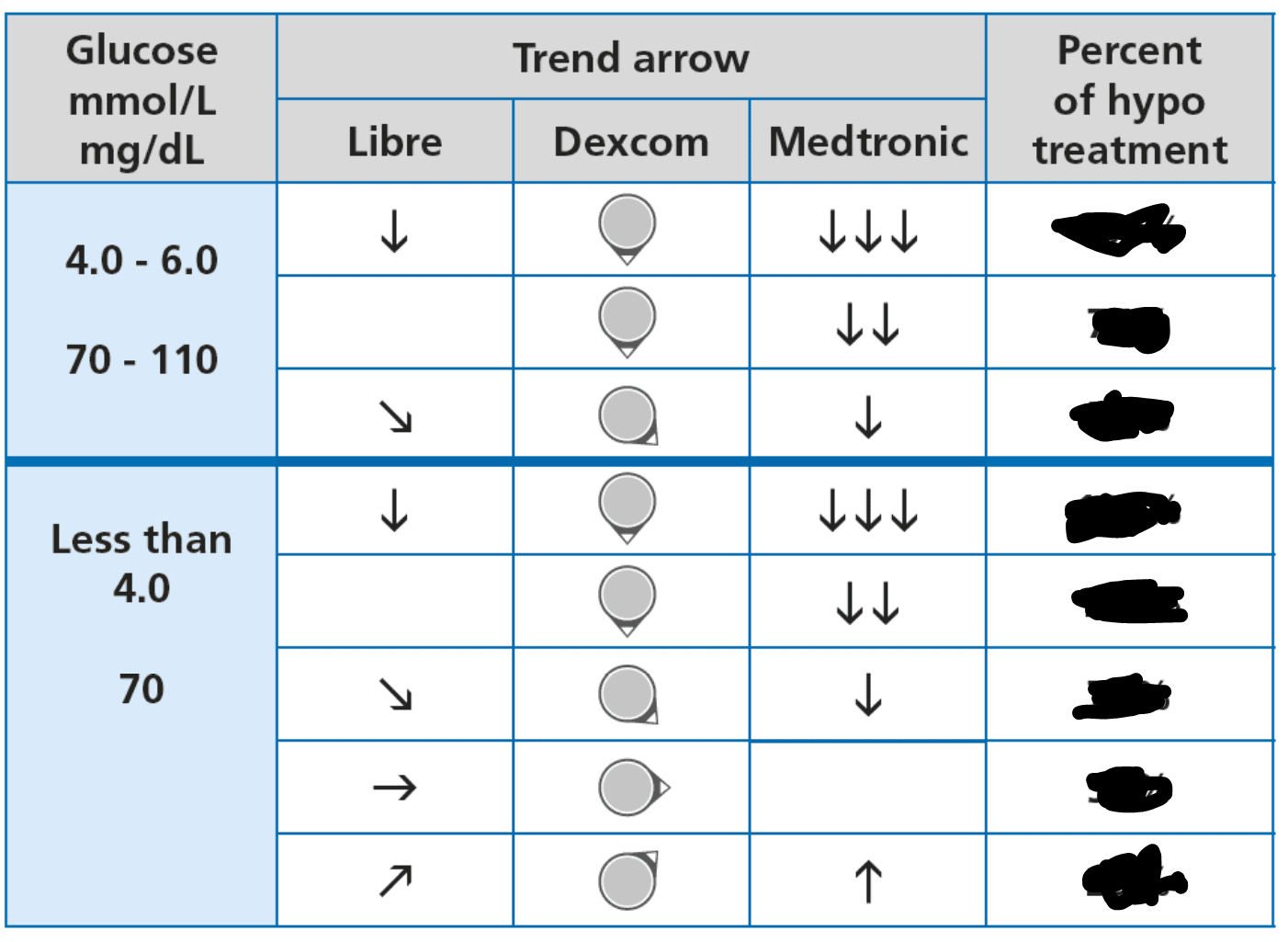
Using trend arrows for prevention
Treatment can differ depending on whether a hypo is already happening or is being prevented, and whether the CGM arrow is flat, single-down, or double-down. The full decision table lives in Dynamic Glucose Management, specifically the MATCH section of GAME-SET-MATCH.
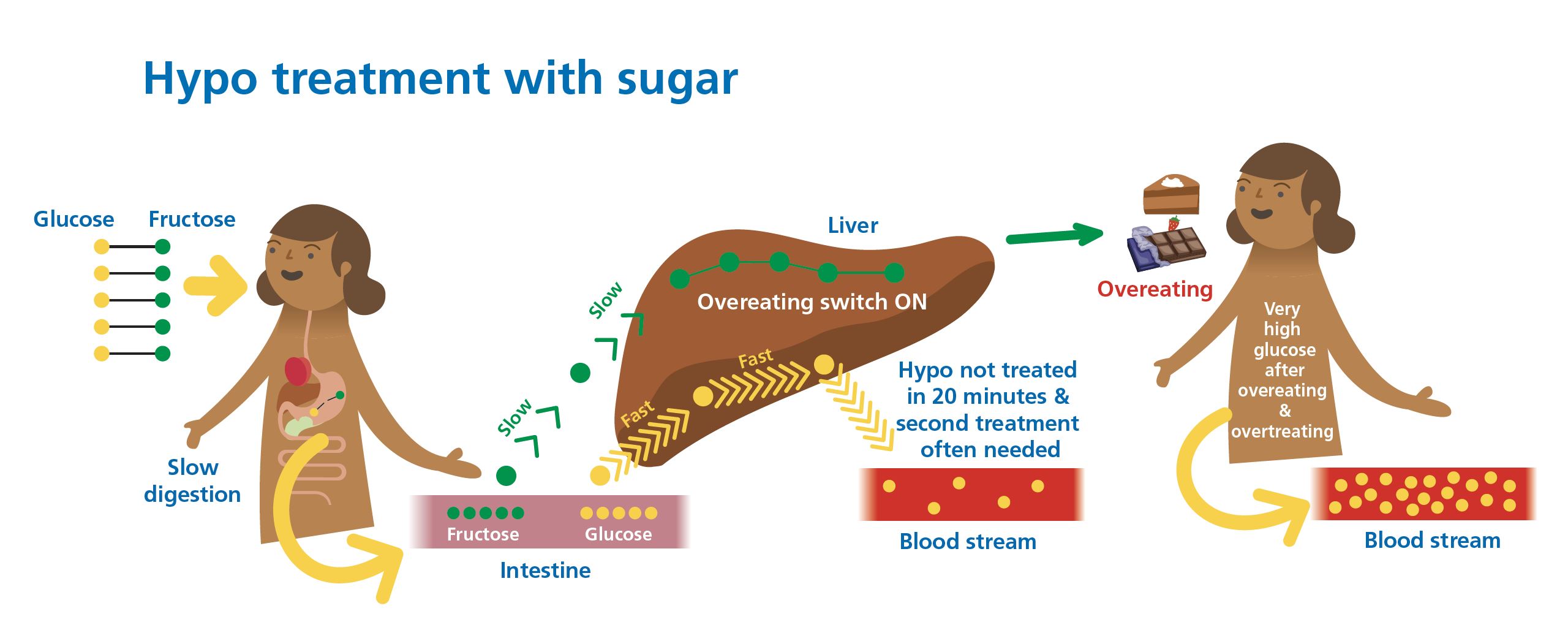
Why sugar treatments overshoot: dose stacking, not pharmacology
A controlled 10 to 15 g dose of sucrose (Skittles in Husband 2010, paediatric RCT) recovers glucose at 15 minutes in 88 per cent of attempts, equivalent to glucose tablets. The common experience of sugar “taking an hour” is driven by dose stacking: larger servings, repeated treatments before the first has been absorbed, and uncounted food eaten alongside. Fructose-heavy treatments (juice, fruit bars) are genuinely slower and fail to recover glucose in about one third of attempts.
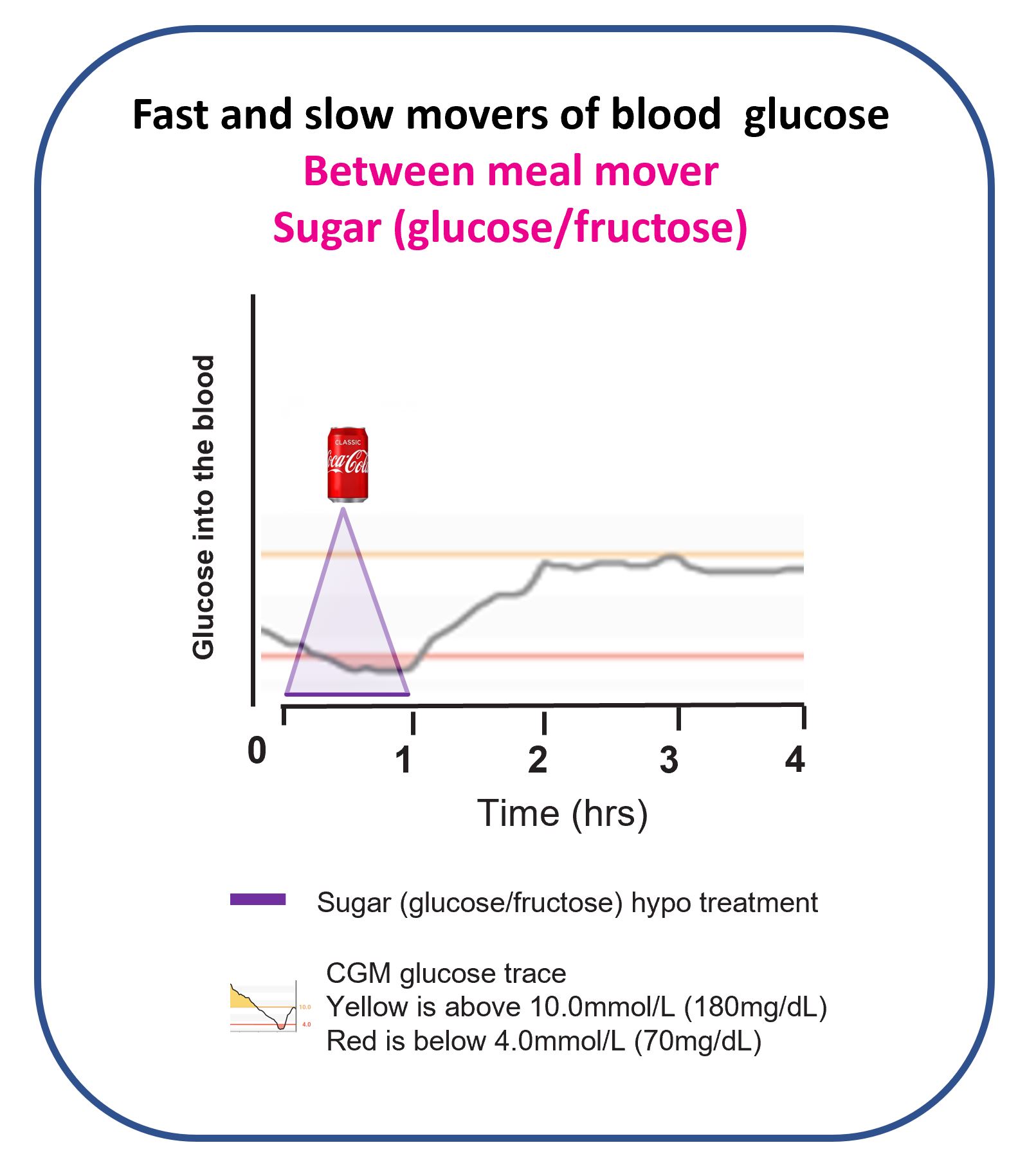
Table sugar (sucrose) is glucose plus fructose in equal parts. At small doses, the glucose half acts quickly and the treatment works. The problem comes when doses are larger or repeated: the fructose half goes to the liver and can trigger hunger and overeating cascades. That is one reason unconstrained sugar treatments so often end in rebound highs; it is a dosing problem, not an inherent problem with sucrose at controlled amounts.
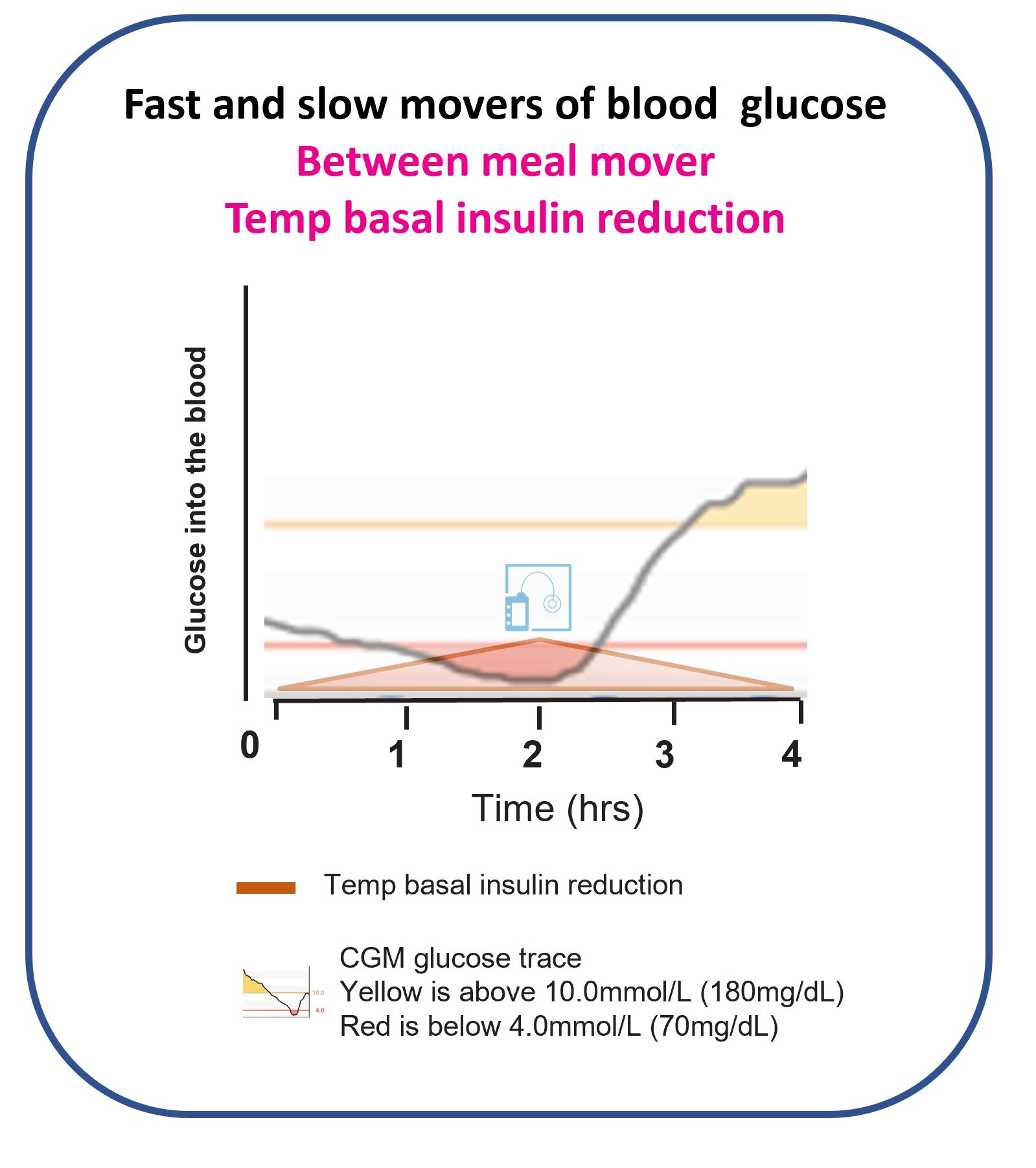
Are temporary basal reductions useful for hypos?
Temporary basal changes are the slowest mover of glucose. They tend to be too delayed to prevent or treat an imminent hypo. This is explored in more depth on the basal insulin page.
Impaired awareness of hypoglycaemia
Around 15 to 30 per cent of adults with type 1 diabetes develop impaired awareness of hypoglycaemia (IAH), where the warning symptoms (shaking, sweating, confusion) become muted or absent. The mechanism is hypoglycaemia-associated autonomic failure (HAAF), set out by Cryer (NEJM 2013): repeated lows blunt the next adrenaline response, which blunts the next set of symptoms, which leads to lower glucose still.
The risk is concentrated. The UK ABCD audit found that a CGM time-below-range above 4 per cent picks up nearly all of those at high severe-hypo risk, and that 4 per cent threshold is now the standard treatment target across ATTD, ADA, and ISPAD.
Awareness can often be restored. Strict avoidance of glucose levels below 4.0 mmol/L for several weeks is sometimes called hypo avoidance or reversing HAAF, and it is one of the strongest arguments for setting CGM alerts conservatively. Worth working through with your diabetes care team.
How AID systems reduce hypoglycaemia
Automated insulin delivery systems with low-glucose suspend or predictive low-glucose management are designed to reduce hypoglycaemia without raising average glucose (Bergenstal, ASPIRE 2013). The German and Austrian DPV registry (Karges 2024, n=13,922) showed that hybrid closed-loop use was associated with a 32 per cent reduction in hypoglycaemic coma, with overall severe hypoglycaemia rates similar to non-HCL care. The 48-month CLOuD extension confirmed that AID does not raise severe-hypo rates over four years of use.
Both findings sit consistently with the broader pattern: AID flattens the worst hypos without trading off elsewhere.
Severe hypoglycaemia: glucagon rescue
Severe hypoglycaemia means the person cannot treat themselves and needs help from someone else. Two glucagon rescue options are now widely available that are significantly easier for bystanders to use than the older reconstitution kits. Tap each for the trial detail.
Intranasal glucagon (Baqsimi)
A single nasal spray, no injection needed. In an induced-hypo crossover (Rickels 2016, n=75), 3 mg intranasal glucagon was non-inferior to 1 mg intramuscular glucagon for raising glucose within 30 minutes (98.7 per cent success vs 100 per cent), with substantially better ease of use under stress.
Glucagon autoinjector (Gvoke)
A pre-filled pen, ready to use without mixing. In simulated rescue with untrained bystanders and trained caregivers (Valentine 2019), the autoinjector achieved 90 per cent or higher correct delivery, compared with very low success on the older Lilly Glucagon Emergency Kit, which required multiple preparation steps under stress.
Discuss a rescue plan with your care team. Everyone who spends time with someone at risk of severe hypoglycaemia should know where the glucagon is and how to use it.
Treating a hypo is medicine, not a snack. Glucose tablets, sized to body weight, rechecked at twenty minutes, repeated only if still low. Trend arrows can scale the dose, and the full matrix lives in Dynamic Glucose Management. Sugar-based alternatives tend to overshoot; that is a dosing problem, not a pharmacology one. Worth working through with your diabetes care team.
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Go deeper: the three-part guide
This page covers the foundations. When you are ready to go further, the three-part Hypoglycaemia Guide picks up where this page stops.
Part 1: Recognising Hypoglycaemia
The two warning systems (adrenergic and neuroglycopenic), what changes when awareness fades, the nocturnal pattern most people only see on the overnight CGM report, and the relative-hypo phenomenon for the high-baseline reader. Anchored on Cryer 2013 (HAAF) and the ABCD audit.
Part 2: Treating Hypoglycaemia
The adult 15-gram rule (Brodows 1984), the paediatric weight-based dose at 0.3 g/kg (McTavish 2011, ISPAD 2024), the glucagon options now available without a reconstitution kit, and how AID changes the protocol after the system has already suspended.
Part 3: Preventing Hypoglycaemia
Four levers in the order they tend to bite: basal review, IOB-aware corrections, sick-day rules, exercise timing. The Optimiser ladder is referenced lightly here; the deep treatment of AID settings lives in the AID guide cluster.
Foundations
Hypoglycaemia