Guide series · Five parts
Exercise and Type 1 Diabetes
Making exercise predictable enough to manage – without pretending it can ever be perfectly controlled. From ten minutes after a meal to training for an endurance event: the same physiology, the same three variables.
TL;DR
- Insulin on board is the dominant driver of exercise hypo risk; the 90-minute window and Three-Hour Rule are how you manage it.
- Activity and exercise are not the same thing. Ten to twenty minutes of everyday movement after meals is a distinct, lower-risk lever for smoothing glucose that most people underuse.
- Three variables decide almost everything: insulin on board, starting glucose, trend arrows. Address these first before adjusting anything else.
- AID changes the levers but not the physics. Announcing exercise and pre-emptive reductions matter more, not less, on an AID system.
- Read Part 3 if you want to understand how twenty minutes of moderate post-meal activity can blunt a postprandial rise without triggering a later hypo.
What this guide is for
Exercise is not random. It is fast physiology meeting slow insulin.
For people living with type 1 diabetes, exercise can feel uniquely destabilising – drops that arrive fast and hard, spikes that linger, sessions that look identical on paper but behave very differently in real life. The common conclusion is that exercise is “unpredictable”. That conclusion is understandable, and usually wrong.
Exercise does not introduce randomness. It introduces fast, powerful physiology into a system otherwise governed by slow, blunt insulin. When you understand the dominant drivers, patterns appear – and with them, a clearer picture.
This guide is built around heuristics to experiment from. Grounded in the evidence base (EASD/ISPAD 2025 consensus, ISPAD exercise chapter, GNL’s own causal modelling), tailored by individual response. They are not rigid rules. They are starting points that survive contact with CGM and real life.
Activity versus exercise
Not all movement requires a full plan
Exercise and everyday activity are not the same thing, and the distinction matters for how you manage glucose.
Activity is everyday movement: walking, light cycling, housework, gardening, playing with children. It is not training. The point is not fitness. The point is glucose leverage. Activity works best as an add-on to normal life – you do not need to be an exercise person to use it.
The contrast matters because the management demands are different:
- Activity: lower hypoglycaemia risk, easier to repeat, well suited to glucose smoothing and post-meal peaks.
- Exercise: higher potential benefit for fitness and performance, but typically requires more deliberate glucose management – before, during, and after.
Starting with activity snacking (ten to twenty minutes after the meal that produces your biggest spike) is often the most accessible entry point, particularly for families and children who find formal exercise management daunting.
Major in the majors
Three variables decide almost everything
If exercise has felt chaotic, start here. Across almost all forms of exercise, glucose behaviour is dominated by three variables, in order of importance.
1 · Most important
Insulin on board
Recent bolus insulin is the dominant driver of exercise hypo risk.
2
Starting glucose
Where you start shapes where you land, especially for aerobic work.
3
Trend arrows
Direction and speed of change. Numbers without direction are incomplete.
When these are prioritised first, exercise stops being mysterious and starts becoming manageable. Most exercise-related hypoglycaemia and volatility is predictable from these starting conditions.
This shows the research-predicted order (which of these best predicts an exercise low). The list above shows what is worth acting on first day to day; insulin on board is what you can most directly change, even where glucose and trend are the stronger predictors.
The core problem exercise creates
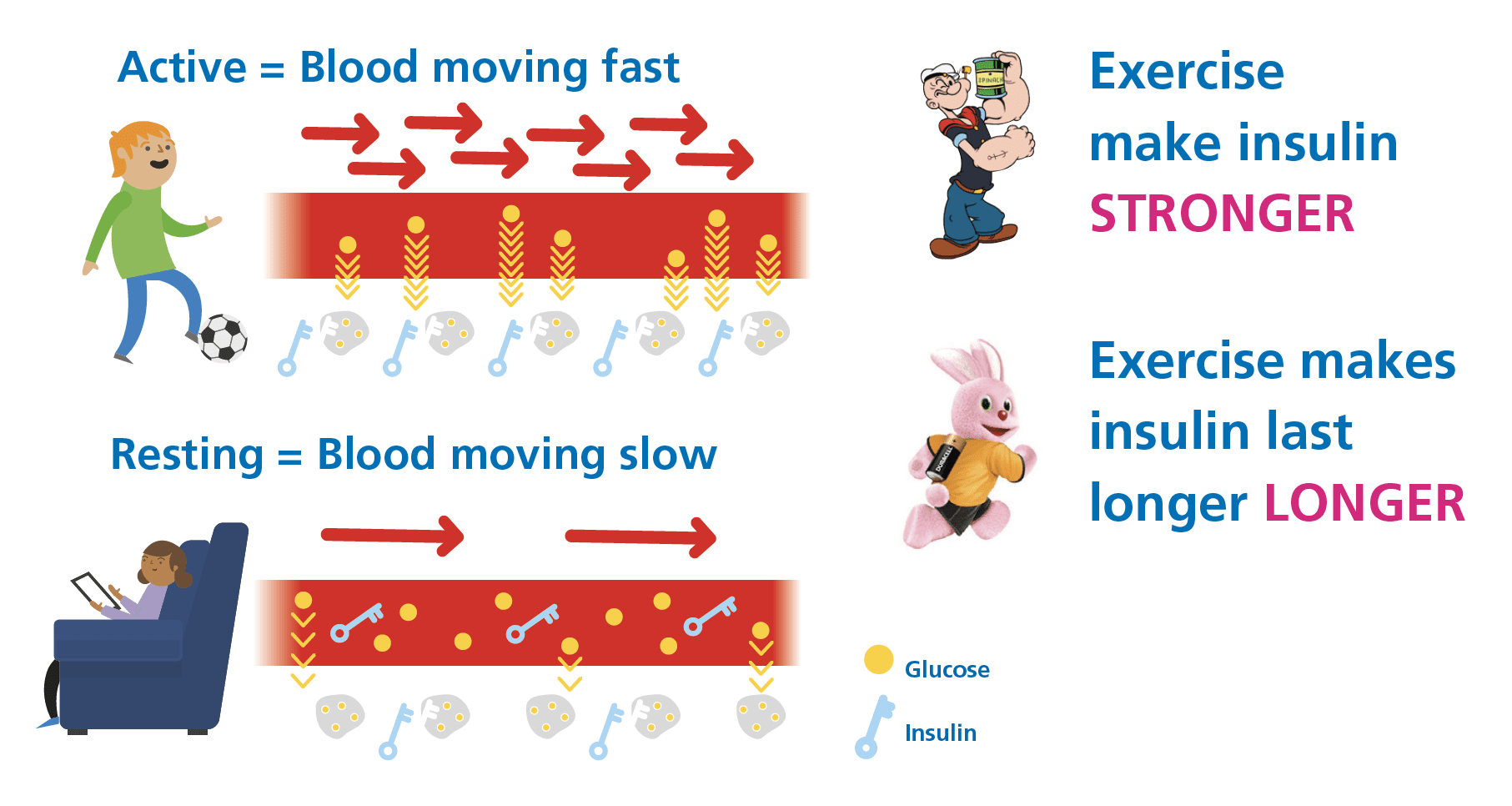
Exercise is hard to manage in type 1 diabetes not because it is dangerous, but because it amplifies insulin action.
Muscle contraction increases glucose uptake. Blood flow accelerates insulin delivery. Counter-regulatory hormones may push glucose out of the liver. These processes act quickly. Injected or pumped insulin does not.
Why exercise hypos are usually insulin problems, not exercise problems
Large glucose drops during exercise are rarely caused by exercise itself. They are almost always caused by supercharged insulin action: exercise increasing blood flow and glucose uptake, amplifying the effect of insulin that is already present. This is physiology doing exactly what it should.
The implication is practical: reducing IOB before exercise (via timing, bolus reduction, or basal adjustment on a pump) addresses the actual cause, not just the symptom.
The 90-minute window explained
When exercise occurs within roughly 90 minutes of a meal bolus, insulin action is often near its peak. In this window, bolus reduction is commonly required to avoid predictable hypoglycaemia. Exercise and peak bolus action overlap.
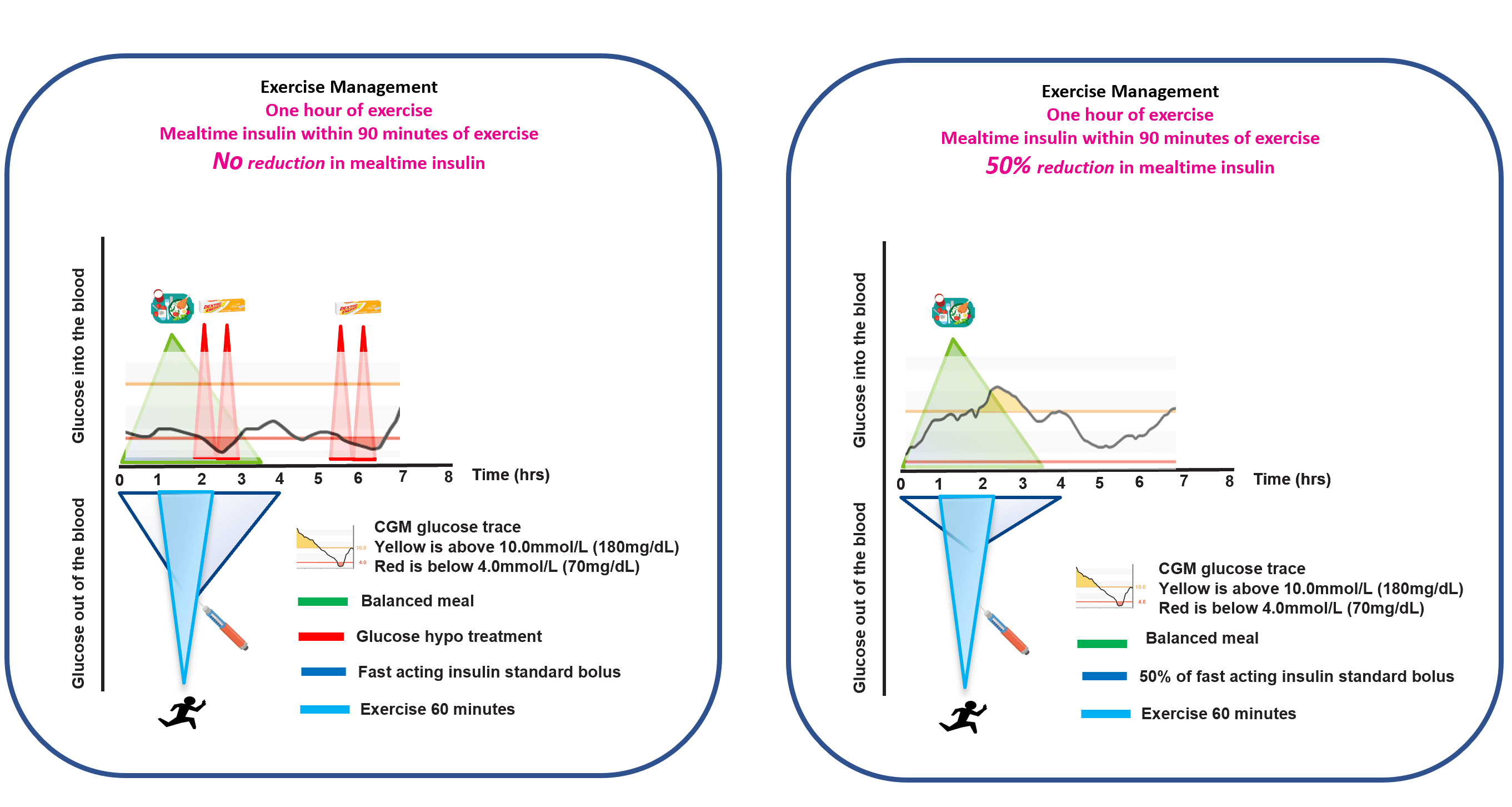
This is also where the activity-versus-exercise distinction matters: a ten-minute walk after a meal sits in this window deliberately and at low enough intensity that hypo risk is lower than with structured exercise.
The reduction protocols: 50/50/20 and T25/T25
Two population-average starting frameworks, one for injections or a pump, one for a hybrid closed loop. Both are teaching simplifications of the graded ISPAD/Rabasa-Lhoret reduction scale, not fixed doses; any insulin change is a care-team decision.
The Three-Hour Rule: what it is and when to use it
One heuristic simplifies exercise management more than almost any other. When the last bolus was at least three hours before exercise, glucose behaviour is often far more predictable.
Not a guarantee. An organising principle that tends to reduce hypos, corrections, and mental load. Worth building exercise timing around where possible.
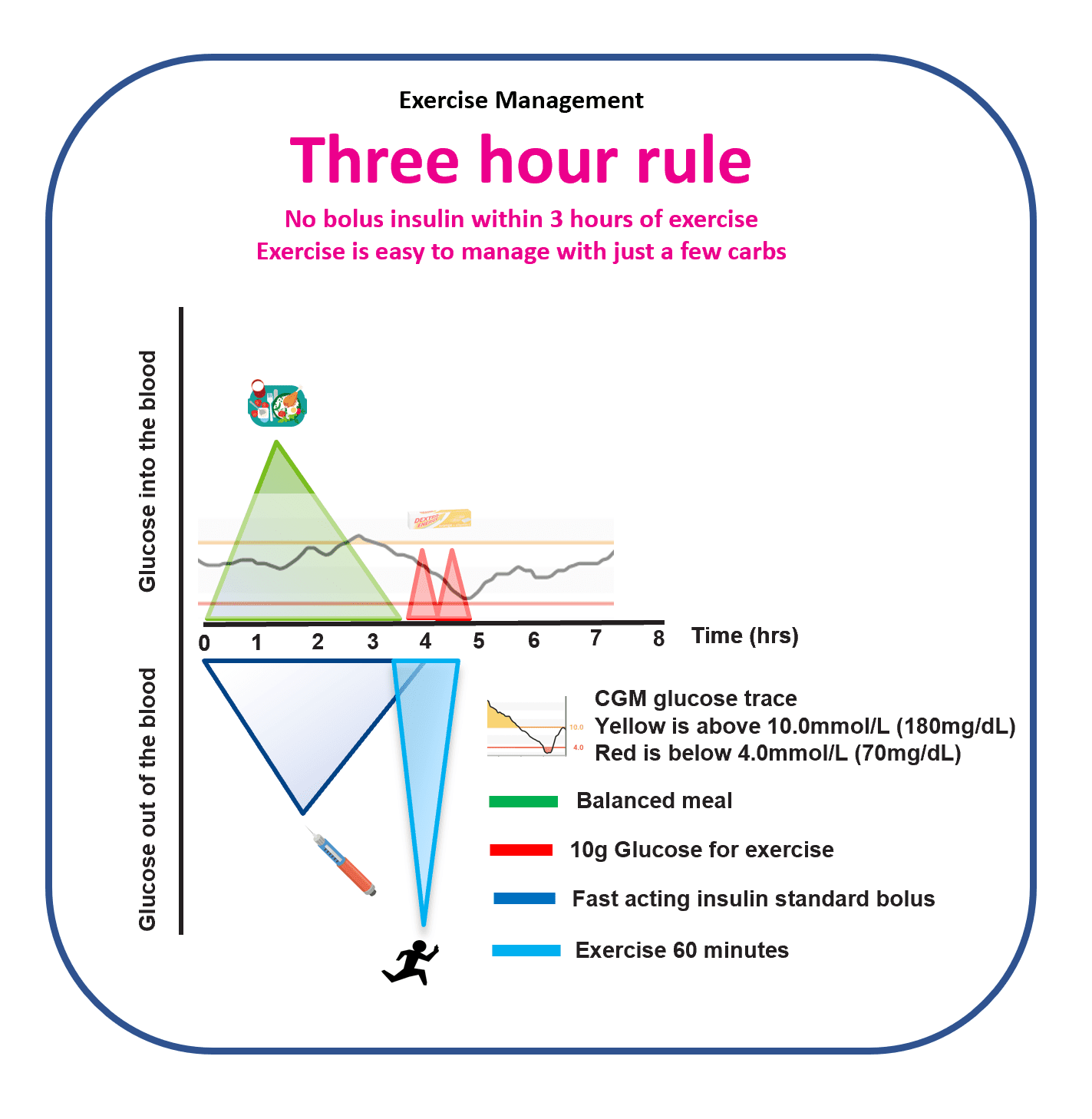
The honest trade: you can have exercise that is more predictable, or you can have exercise that fits life as it actually arrives. The Three-Hour Rule and the 90-minute window are levers, not gates. Most days you will choose flexibility; on the days the stakes are higher (long ride, race, mountain), the rule is there to lean on.
Activity snacking
Ten minutes after meals: the most underused lever in T1D
A short walk after meals is one of the most underrated tools in type 1 diabetes management. Movement creates glucose uptake demand at exactly the time glucose is rising from a meal. The result tends to be a lower post-meal peak and a gentler curve, without adding complexity to an exercise management plan.
- Starting with ten minutes after the meal that produces your biggest spike is a practical entry point.
- A pace you can repeat daily works better than an ambitious pace you cannot sustain.
- CGM provides the feedback: you are looking for a lower peak and a gentler descent.
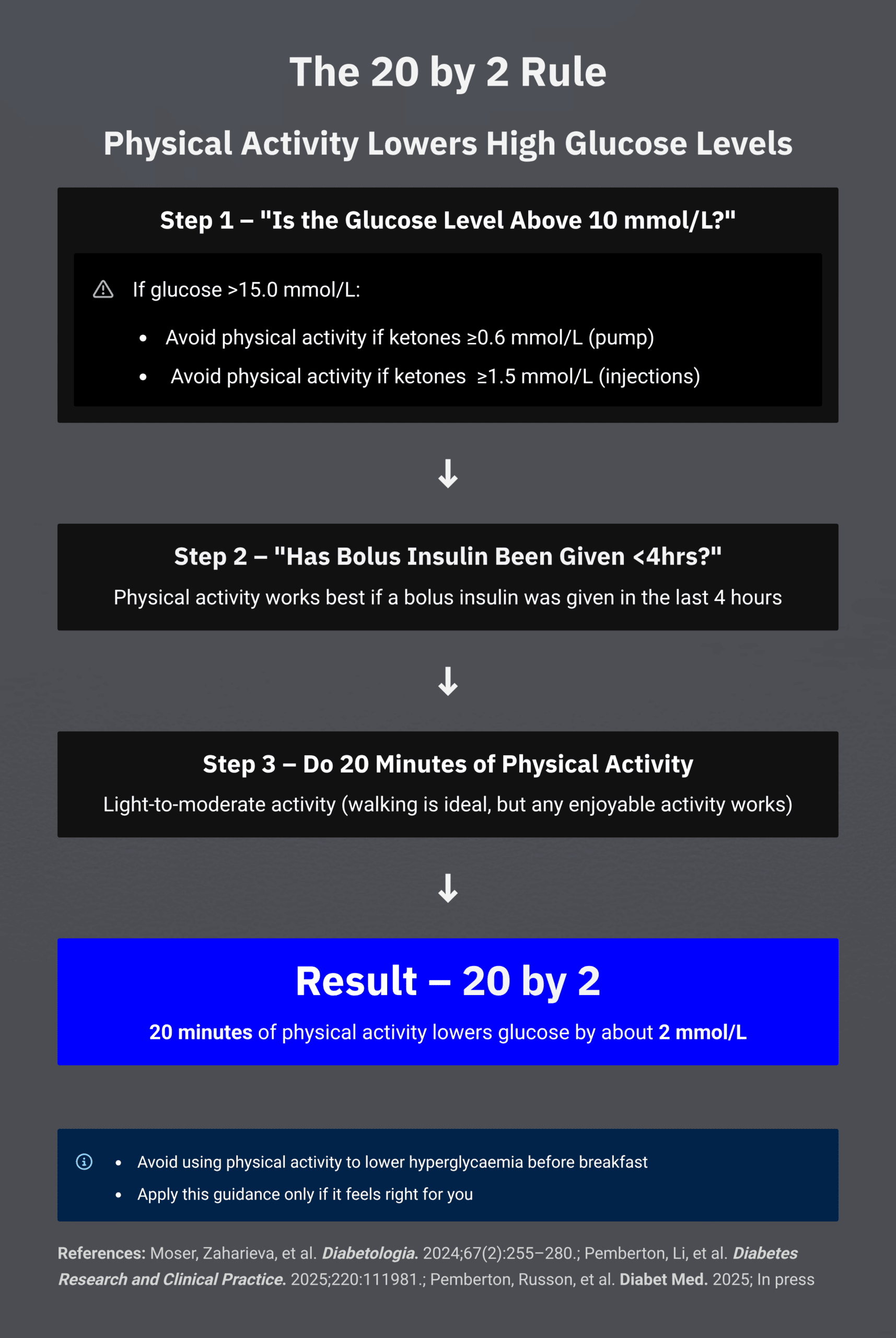
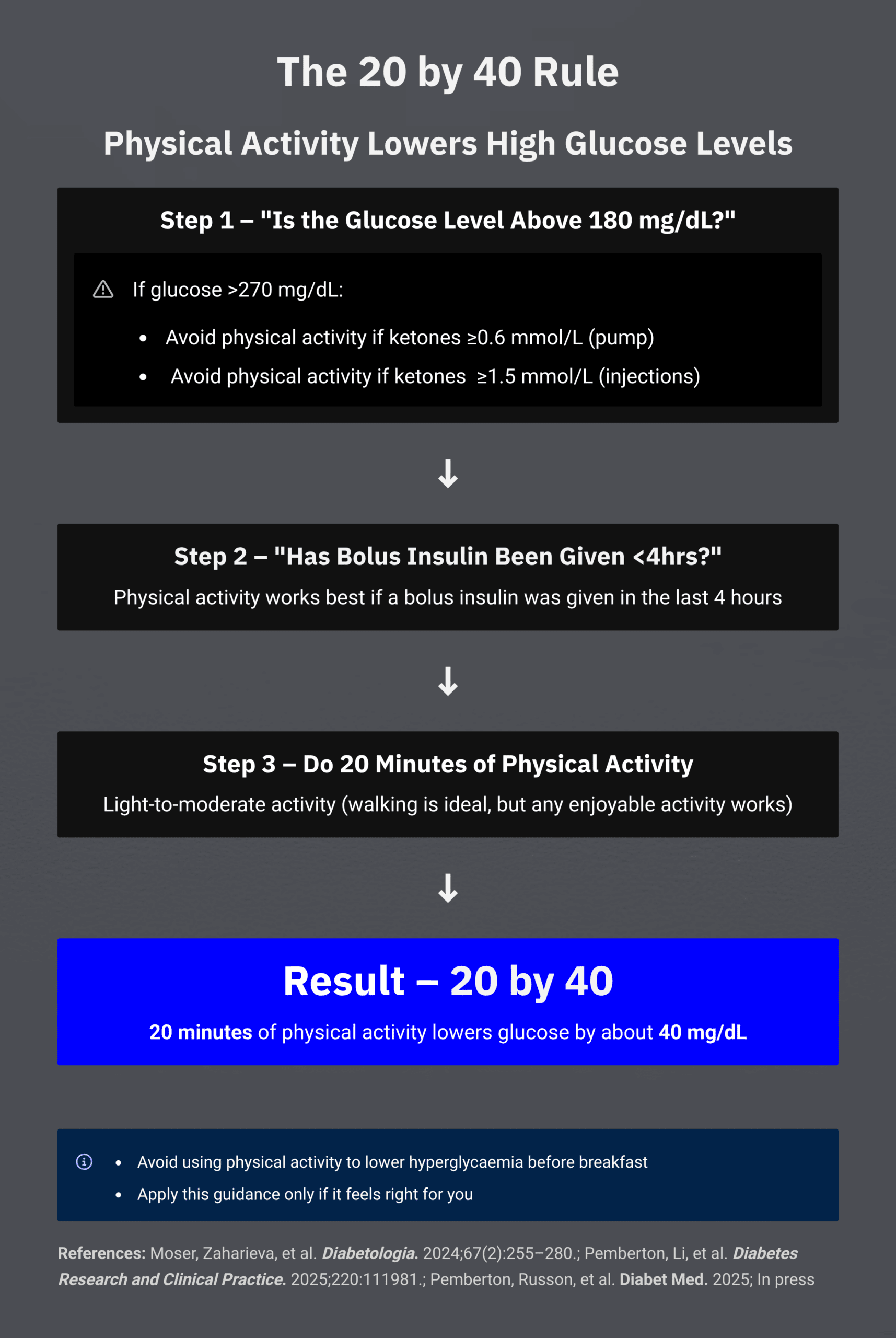
Activity snacking when glucose is elevated between meals (20 by 2 and 20 by 40)
Light activity amplifies the effect of insulin already on board. For some people, this can meaningfully lower glucose without stacking further insulin corrections – particularly in the window when a previous meal bolus is still active. This is not a replacement for insulin when insulin is needed; it is a tool for the right situation.
- Twenty minutes of light activity can lower glucose meaningfully for many people.
- Activity is not appropriate when ketones are elevated; in that situation, sick-day rules apply.
- Individual response size and timing vary; CGM is the tool for observing your own pattern.
The GNL Activity Snacking (20 by 2) approach describes this in more depth. Download the reference sheets: 20 by 2 (PDF) and 20 by 40 (PDF).
In Grace’s words: “99 problems, but highs ain’t one.”
Fast movers and slow movers: knowing which you are
Activity does not just “burn glucose”; it amplifies insulin action. Some people experience a rapid glucose fall with even light movement because activity dramatically boosts the effect of insulin already on board (fast movers). Others see a slower or smaller response because there is less active insulin to amplify.
Knowing the approximate amount of insulin on board helps with dosing movement and optimising time in range. Explore further: Fast and slow movers, understanding your individual activity response.
CGM as activity biofeedback: what to look for
CGM makes activity more useful because it converts vague advice (“be more active”) into visible, real-time feedback. The signals to look for are:
- lower post-meal peaks,
- less time spent in the high range,
- fewer correction cycles needed.
For families, CGM has an additional benefit: children can see movement changing glucose in real time, which tends to build confidence and reduce fear around activity.
See the full CGM series: CGM Series, How to Choose a CGM.
What GNL research shows
The 20-minute paradigm
Pemberton et al (2024, 2025) identified that twenty minutes of moderate activity, timed into the post-meal window, is often enough to blunt a postprandial rise without triggering a later hypo – provided insulin on board and trend direction are accounted for. This reframes activity from an all-or-nothing risk to a precision tool. Developed further in Pemberton & Russon (2025) causal modelling work. Covered in depth in Part 3.
The five parts
Read in order for the full picture, or jump to the Part closest to your question. Every Part opens with the same “major in the majors” framing, so you can skip between them without losing your bearings.
Part 1
How exercise moves glucose
Mechanism, exercise types, the three majors, the 90-minute window, the Three-Hour Rule. The physiology that sits underneath every other Part.
Part 2
The two levers – insulin and carbs
Bolus reductions (the 25/50/75% framework), carb timing and amounts, fasted versus fed, pump disconnection, and the evidence from Rabasa-Lhoret, Moser, West, Campbell, and Riddle.
Part 3
Activity between meals – the 20-minute paradigm
John’s research on postprandial activity: when, why, and how twenty minutes can shift a day. Pre-meal versus post-meal walking. Sitting breaks. The evidence for activity snacking in both children and adults.
Part 4
AID and exercise
What AID can and cannot do during exercise. Announce strategies, 30-minute activity features, manual mode trade-offs, pre-emptive carbs and reductions. Based on the Moser/Zaharieva EASD/ISPAD 2025 consensus.
Part 5
Mastering Exercise – Top 10
Ten tactics that survive contact with real-world exercise and real CGM data. CGM accuracy during exercise, sex differences, fear of hypo, altitude, barriers and facilitators, T1DeXi and Syno/MIMIC insights.
Explorers and tools
Three GNL explorers are built directly on the evidence and algorithms in this guide.
- 10, 20, 30 Minutes Walking to Lower Highs – the activity-snacking tool that pairs with Part 3
- Carbs for 30 Minutes Exercise – the exercise IOB calculator that pairs with Part 2
- Planning for Before, During and After Exercise – the full planning explorer that pulls all five Parts together
Survive and Thrive – Exercise resources
Three one-page A4 resources built for the first weeks of getting exercise predictable. Pick the one that matches your therapy.
Further listening and related content
- FAQ – Activity, Exercise and Type 1 Diabetes
- Podcast with Prof Othmar Moser on exercise and T1D
- Episode 33 – Exercise, hormones and T1D in females
- The Menstrual Cycle and Type 1 Diabetes, three-part guide: cycle physiology, AID across the cycle, contraception, PCOS, pregnancy, and menopause
- Foundations – Activity and Movement
- CGM and exercise: bolus reduction and carbohydrate timing
- Fast and slow movers, understanding your individual activity response
- Activity Snacking (20 by 2)
- Hypoglycaemia in T1D – understanding and preventing lows
Pairs with the CGM and AID guides
Exercise, CGM, and AID are one decision system. If you are planning for all three, start with the guide you have not yet read.
For competitive athletes, a bespoke service
If you (or your child) are training for an Ironman, marathon, rowing championship, cycling stage race or similar endurance event, and want a personalised plan that combines paediatric T1D clinical expertise, sports nutrition, pump-data interpretation and AI-augmented in-the-moment support, John runs a bespoke Athlete Performance service through Via Negativa Health. Free 60-minute sound-out call before any engagement.
Keep reading
This guide is educational. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.