Mealtime Insulin Guide, Part 2 of 3
Balanced Meals: Stay in Range
It is Tuesday evening, the family is sat down, the plate is half vegetables, a palm of chicken, a fist of rice. Twenty minutes ago you pre-bolused on the way to the kitchen. The CGM line is climbing gently, peaks somewhere around 8.5 mmol/L, and is back near baseline by the time you load the dishwasher. Nothing dramatic happened. That is the point. Balanced meals are the workhorse of staying in range; they make insulin timing predictable enough to learn from.
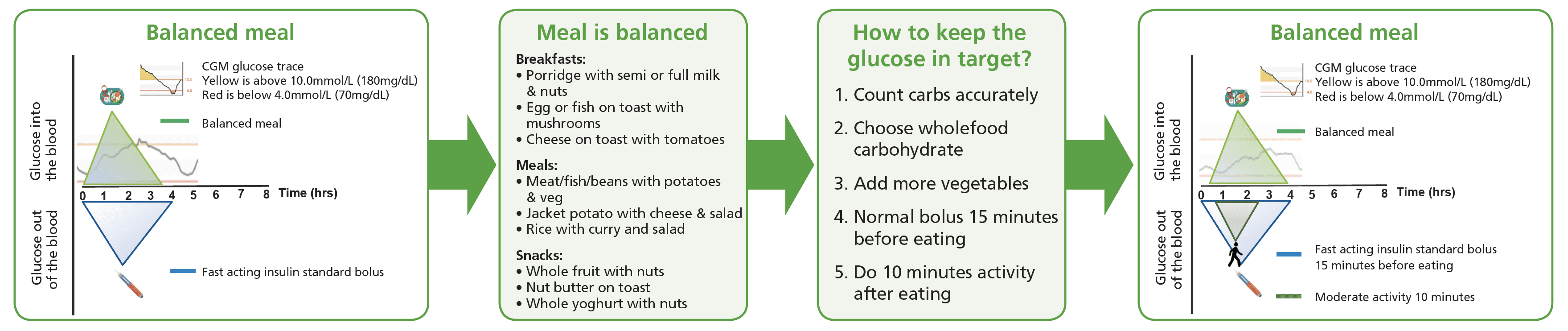
What a balanced plate looks like
Half the plate vegetables, a quarter protein, a quarter carbohydrate. A palm of meat, fish, or beans for the protein. A fist of potatoes, rice, pasta, or bread for the carb. The vegetables do not need to be exotic; whatever the family will actually eat, prepared in a way that does not need a chef. As snacks: whole fruit with a handful of nuts, full-fat yoghurt with seeds, nut butter on toast.

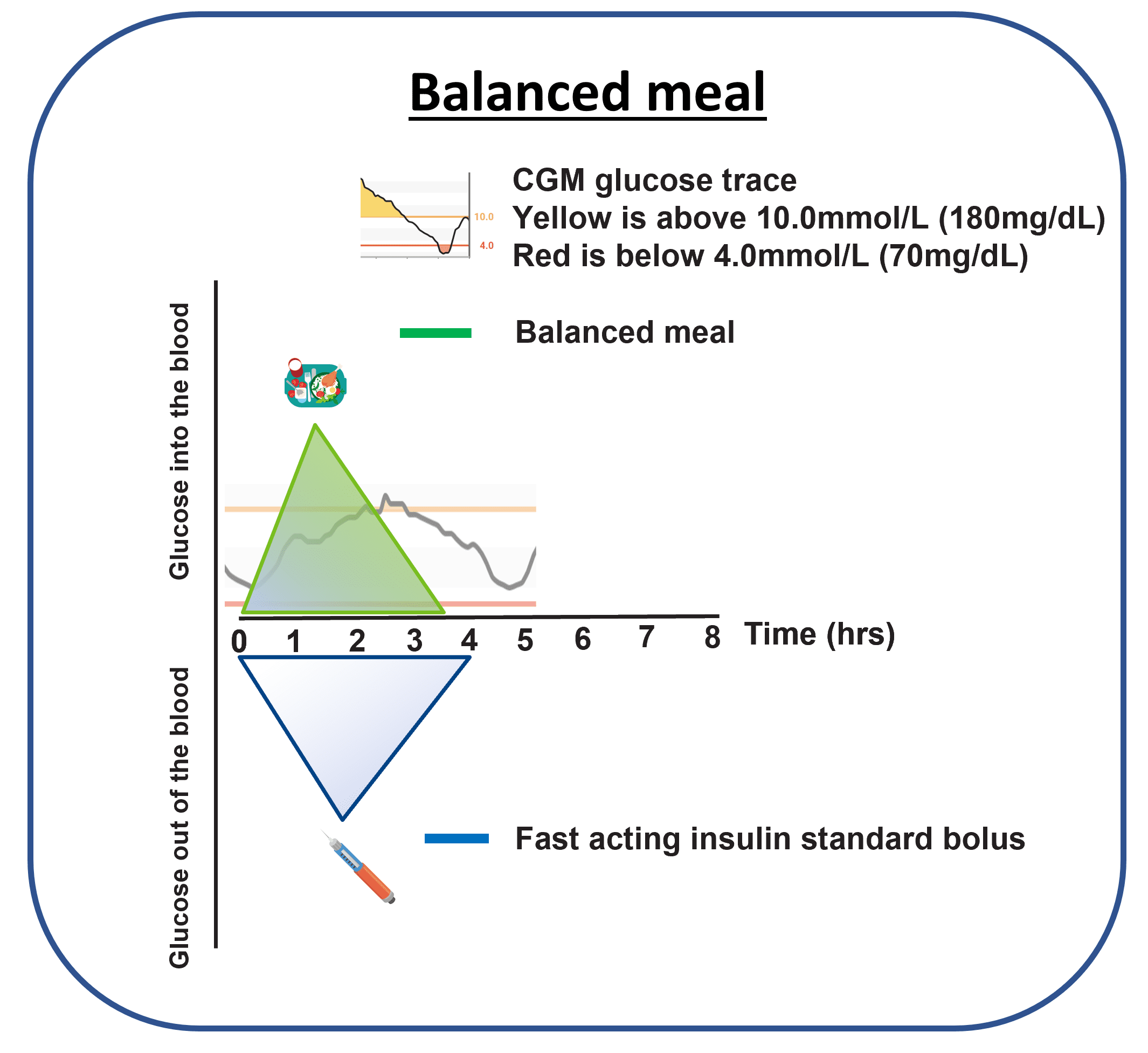
What the trace tends to look like
Balanced meals produce a smaller, slower glucose rise than high-carb meals. The protein, fat, and fibre slow gastric emptying; the smaller carbohydrate fraction does not flood the bloodstream; the insulin has time to come on board and meet the meal. A spike can still appear if the bolus arrives late, but the magnitude of the miss is smaller and the recovery faster.
Why a spike can still happen
The same two structural reasons from Part 1 still apply: the missing portal-vein signal means the liver brake is weaker than it would be without diabetes, and subcutaneous insulin still takes tens of minutes to start working. The reason balanced meals feel kinder is that digestion is slower, so the gap matters less. If the dose lands on time the curve flattens; if it lands late, you get a small version of the same mismatch the high-carb page describes.
The two SET moves that flatten the curve
The moves are the same as on Part 1, because the underlying problem is the same. On a balanced meal, both moves do less heavy lifting because the meal is doing more of the work; that is exactly why the combination is so reliable on this kind of plate.
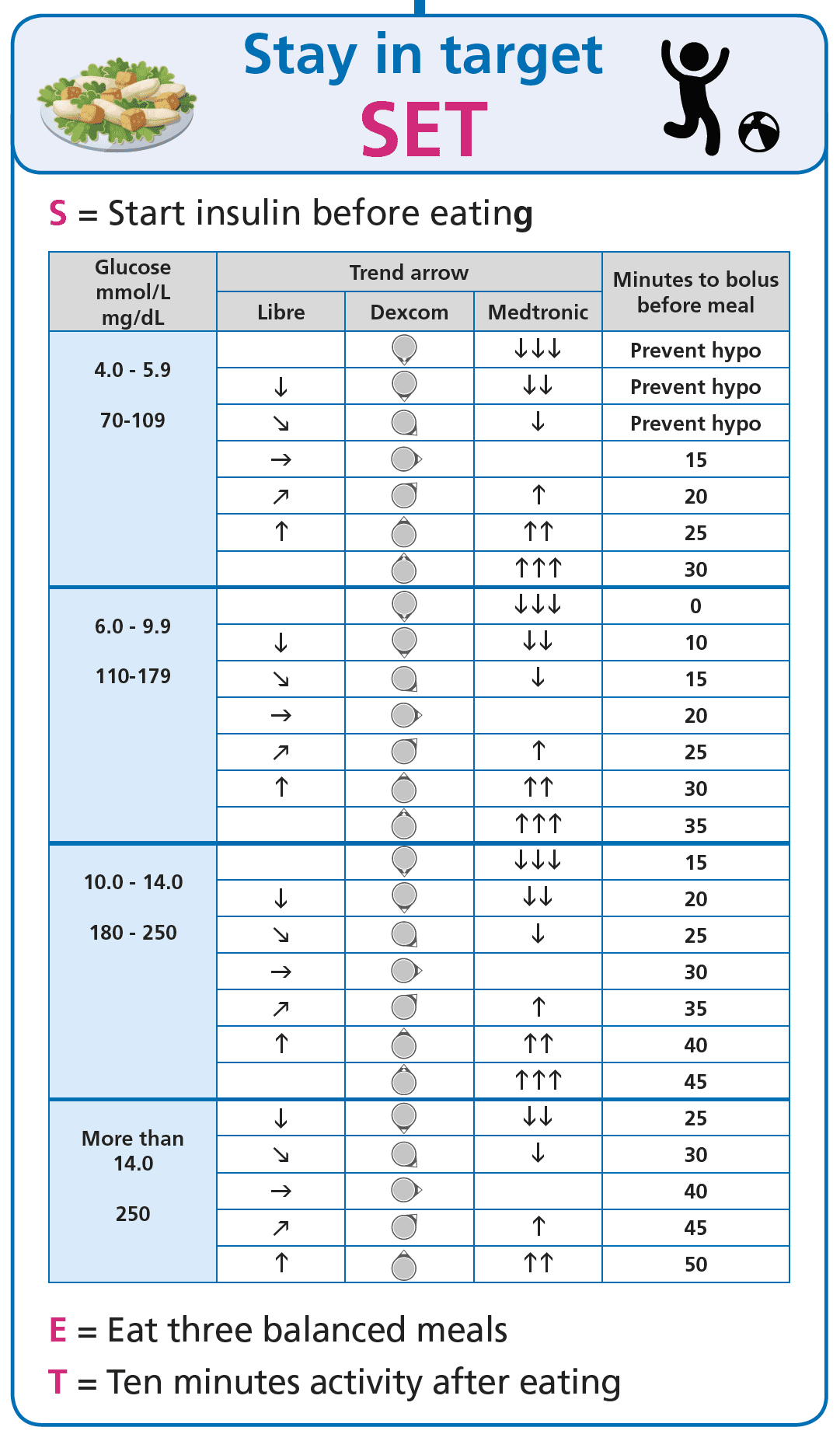
The S, state-based pre-bolus timing
Give insulin a head start by pre-bolusing on the way to the kitchen. The window is around 20 minutes on a standard rapid analogue from a glucose in the target range; shorter if the starting glucose is low, longer if it is high; shorter or none on the ultra-rapid analogues. State-based means the window is read off the CGM, not from a recipe card.
The T, ten minutes of light activity after eating
A walk to clear the table, the dishes, the school-run pavement. Muscle uptake of glucose increases sharply with even gentle movement and the post-meal peak comes down. Of all the moves on this page, the post-meal walk is the one with the lowest cost and the most reliable effect.
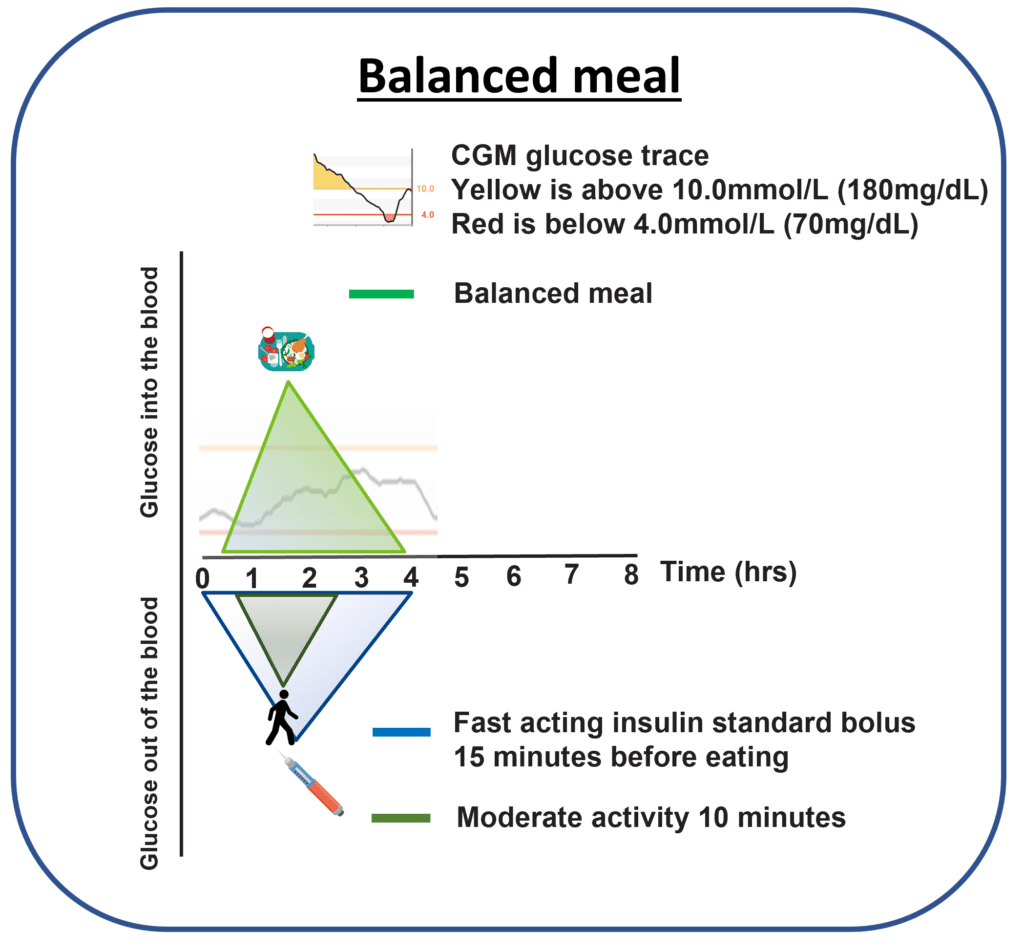
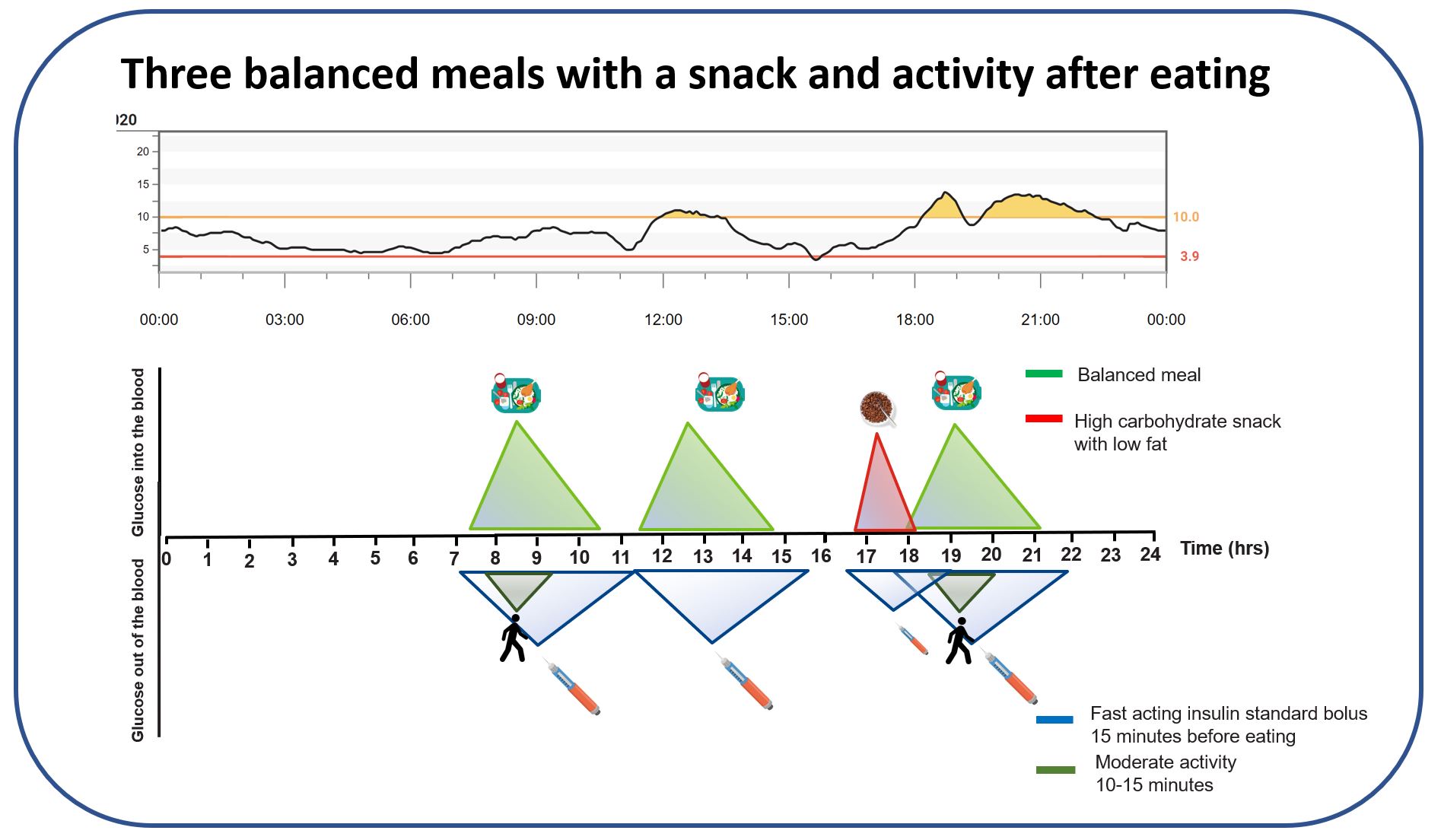
The strategy in one picture
For the readers who learn best from a single image rather than a page of prose, the same content as the disclosures, condensed.
What tends to follow when this is the baseline
When balanced meals are the everyday baseline and the post-meal walk is feasible most of the time, very high time in range stops feeling like a stretch. From the GNL community and from the conversations I have in DAFNE, around 85 percent time in range is a common outcome on this baseline, without diabetes consuming the day. Population-average pattern; individual response varies; your numbers belong to you and your diabetes care team.
Balanced meals make insulin timing predictable enough to learn from. Half veg, a palm of protein, a fist of carb keeps the meal inside the window the carb ratio was tuned for. Pre-bolus and post-meal movement flatten the curve from there. The point is not that every meal must be balanced; the point is that the more your week looks like this, the more reliable everything else becomes.
This content is for educational exploration only. The 85 percent time-in-range figure is a population-average observation in people who have the structural baseline in place; individual targets sit with your diabetes care team.
Trying it on a meal you already eat
Pick a meal that already lands roughly on the plate model (the Sunday roast, the weeknight stir-fry, the chicken-and-veg lunchbox). Run it twice. The first time, do nothing different and watch the trace. The second time, pre-bolus 20 minutes ahead and walk for 10 minutes after. The CGM is the answer; the glucose never lies. Bring both traces to your diabetes care team if the second trace still climbs above target; the conversation is then anchored in your data, not in averages.
References
Slattery 2018, optimal prandial bolus timing review
Slattery D, Choudhary P. Clinical use of continuous glucose monitoring in adults with type 1 diabetes, optimal prandial bolus timing. Diabetic Medicine. 2018. The clinical literature anchor for the 20-minute pre-bolus on rapid analogues for usual mixed meals.
Pemberton 2021, Mealtime Insulin Guide (the wider matrix this part sits inside)
Pemberton J, et al. The Glucose Never Lies Mealtime Insulin Guide for type 1 diabetes. Pediatric Diabetes. 2021. COI flag: John Pemberton is lead author. Anchors the dosing matrix on the Mealtime Insulin hub; the usual mixed-meal pattern (40 to 55 percent carbohydrate by energy) is the window the carb ratio was tuned around.
Pemberton 2019, KISS audit at Birmingham Women’s and Children’s NHS FT
Pemberton J, et al. Keep It Super Simple: a structured-education audit. Pediatric Diabetes. 2019. COI flag: John Pemberton is lead author. The clinic-level evidence behind the structural-baseline approach to balanced eating.
Part 2 of 3
Balanced Meals: Stay in Range